Rosalinde A L Smits, Bas F M van Raaij, Steffy W M Jansen, Jessica M van der Bol, Carolien M J van der Linden, Harmke A Polinder-Bos, Hanna C Willems, Ewout W Steyerberg, Maarten van Smeden, Jacobijn Gussekloo, Simon P Mooijaart, Stella Trompet
{"title":"Validation of the acutely presenting older patient screener for short term mortality prediction in older patients hospitalized for COVID-19.","authors":"Rosalinde A L Smits, Bas F M van Raaij, Steffy W M Jansen, Jessica M van der Bol, Carolien M J van der Linden, Harmke A Polinder-Bos, Hanna C Willems, Ewout W Steyerberg, Maarten van Smeden, Jacobijn Gussekloo, Simon P Mooijaart, Stella Trompet","doi":"10.1007/s41999-025-01200-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The aim of this study was to validate the acutely presenting older patient (APOP) screener, routinely used on the Emergency Department to predict risk of adverse outcomes in older people, for prediction of in-hospital mortality and 30-days-mortality in older patients hospitalized for COVID-19.</p><p><strong>Methods: </strong>Patients ≥ 70 years from a multicenter cohort hospitalized for COVID-19 with measured APOP risk were included. External validation analysis of the APOP screener for in-hospital mortality and 30-days-mortality was performed including discrimination and calibration.</p><p><strong>Results: </strong>389 patients (median age 80 (IQR 75-85) years, 41.4% female, 138 APOP high risk) were included. APOP high risk patients more often lived institutionalized, (26% vs. 4%; p < 0.001), had more comorbidities (Charlson Comorbidity Index 2 (1-3) vs. 2 (0-3); p = 0.002) and were less often fit (Clinical Frailty Scale 1-3 17% vs. 62%; p < 0.001). 84 patients died in hospital and 114 within 30 days. APOP high risk patients had a higher risk of in-hospital-death [OR 1.6 (95% CI 1.0-2.6)] and death within 30 days [OR 2.7 (95% CI 1.7-4.2)]. The APOP screener discriminated poorly for in-hospital mortality [AUC 0.56 (95% CI 0.48-0.63)] and for 30-days-mortality [AUC 0.62 (95% CI 0.55-0.68)]. Calibration plots revealed overestimation of the screener for both mortality risks.</p><p><strong>Conclusion: </strong>The APOP screener had a poor predictive performance for in-hospital mortality and 30-days-mortality in older people hospitalized for COVID-19. Screening tools routinely used on the ED may not be useful to predict mortality in different than usual clinical circumstances such as during a pandemic of a novel disease.</p>","PeriodicalId":49287,"journal":{"name":"European Geriatric Medicine","volume":" ","pages":"1519-1526"},"PeriodicalIF":3.6000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12378732/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Geriatric Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s41999-025-01200-4","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/22 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: The aim of this study was to validate the acutely presenting older patient (APOP) screener, routinely used on the Emergency Department to predict risk of adverse outcomes in older people, for prediction of in-hospital mortality and 30-days-mortality in older patients hospitalized for COVID-19.
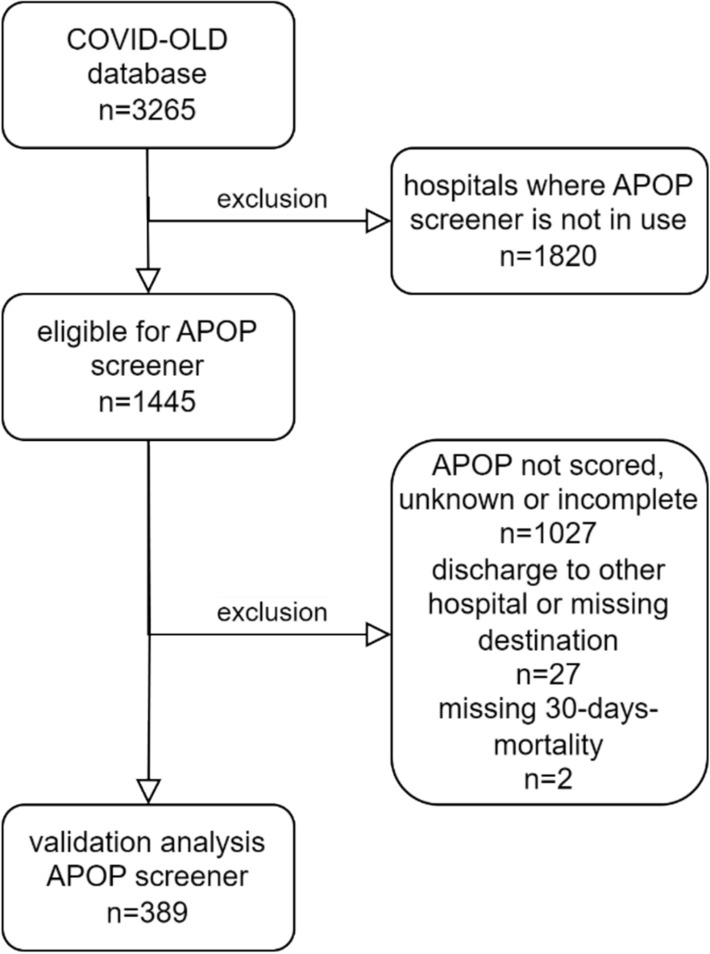
Methods: Patients ≥ 70 years from a multicenter cohort hospitalized for COVID-19 with measured APOP risk were included. External validation analysis of the APOP screener for in-hospital mortality and 30-days-mortality was performed including discrimination and calibration.
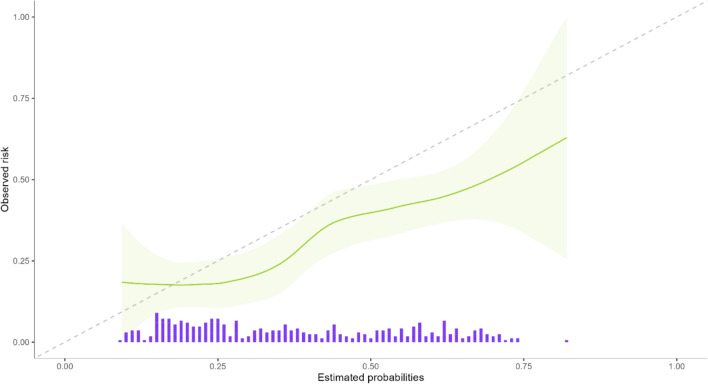
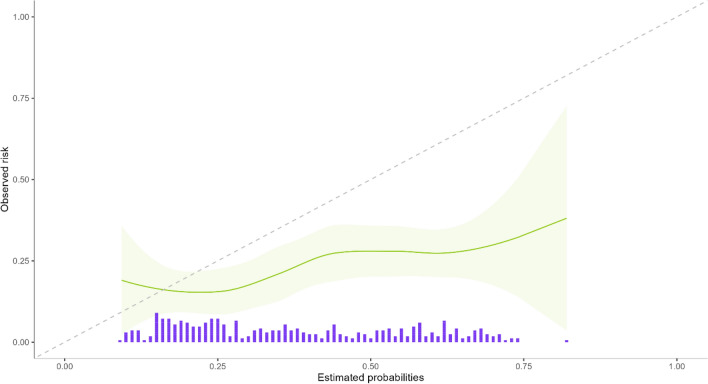
Results: 389 patients (median age 80 (IQR 75-85) years, 41.4% female, 138 APOP high risk) were included. APOP high risk patients more often lived institutionalized, (26% vs. 4%; p < 0.001), had more comorbidities (Charlson Comorbidity Index 2 (1-3) vs. 2 (0-3); p = 0.002) and were less often fit (Clinical Frailty Scale 1-3 17% vs. 62%; p < 0.001). 84 patients died in hospital and 114 within 30 days. APOP high risk patients had a higher risk of in-hospital-death [OR 1.6 (95% CI 1.0-2.6)] and death within 30 days [OR 2.7 (95% CI 1.7-4.2)]. The APOP screener discriminated poorly for in-hospital mortality [AUC 0.56 (95% CI 0.48-0.63)] and for 30-days-mortality [AUC 0.62 (95% CI 0.55-0.68)]. Calibration plots revealed overestimation of the screener for both mortality risks.
Conclusion: The APOP screener had a poor predictive performance for in-hospital mortality and 30-days-mortality in older people hospitalized for COVID-19. Screening tools routinely used on the ED may not be useful to predict mortality in different than usual clinical circumstances such as during a pandemic of a novel disease.
期刊介绍:
European Geriatric Medicine is the official journal of the European Geriatric Medicine Society (EUGMS). Launched in 2010, this journal aims to publish the highest quality material, both scientific and clinical, on all aspects of Geriatric Medicine.
The EUGMS is interested in the promotion of Geriatric Medicine in any setting (acute or subacute care, rehabilitation, nursing homes, primary care, fall clinics, ambulatory assessment, dementia clinics..), and also in functionality in old age, comprehensive geriatric assessment, geriatric syndromes, geriatric education, old age psychiatry, models of geriatric care in health services, and quality assurance.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


