{"title":"Pneumoperitoneum Caused by a Ruptured Splenic Abscess Mimicking Gastrointestinal Perforation: A Case Report.","authors":"Naoki Kawahara, Mitsuaki Kojima, Koji Morishita","doi":"10.70352/scrj.cr.24-0098","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Splenic abscess is a rare but potentially life-threatening condition that can rupture, leading to pneumoperitoneum and symptoms that mimic gastrointestinal perforation in rare cases. This can significantly complicate accurate diagnosis and prompt treatment. A splenic abscess can become life-threatening by rupturing, which may cause diffuse peritonitis or sepsis.</p><p><strong>Case presentation: </strong>A 68-year-old man with uncontrolled diabetes presented with fever, chills, and abdominal pain. Initial evaluation at a previous hospital, including computed tomography (CT), suggested a lower gastrointestinal perforation, leading to his transfer to our facility. CT revealed a non-enhancing lesion with gas in the spleen and free intraperitoneal air; however, there was no clear evidence of gastrointestinal perforation. An emergency exploratory laparotomy was performed, which revealed purulent ascites and a ruptured splenic abscess without any gastrointestinal perforation. After thorough lavage to eliminate contamination, open abdominal management was initiated owing to a need for catecholamine support and an inability to completely rule out the possibility of gastrointestinal perforation. A second-look laparotomy confirmed that there was no further contamination or gastrointestinal tract perforation. Blood and abscess cultures revealed <i>Escherichia coli</i>, leading us to initiate targeted antibiotic therapy. The patient recovered successfully and was discharged on postoperative day 40 without any recurrence. Ruptured splenic abscess with pneumoperitoneum is rare and poses significant diagnostic challenges, particularly in patients with diabetes, owing to its clinical similarity to gastrointestinal perforation. This study highlights the utility of exploratory laparotomy and staged open abdominal management when gastrointestinal perforation cannot be ruled out.</p><p><strong>Conclusions: </strong>Physicians should consider ruptured splenic abscesses in patients with pneumoperitoneum, particularly those with diabetes. Exploratory laparotomy with staged open abdominal management may represent an effective approach that facilitates safe monitoring and targeted treatment, thereby reducing the risk of fatal complications.</p>","PeriodicalId":22096,"journal":{"name":"Surgical Case Reports","volume":"11 1","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12066237/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.70352/scrj.cr.24-0098","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/25 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Splenic abscess is a rare but potentially life-threatening condition that can rupture, leading to pneumoperitoneum and symptoms that mimic gastrointestinal perforation in rare cases. This can significantly complicate accurate diagnosis and prompt treatment. A splenic abscess can become life-threatening by rupturing, which may cause diffuse peritonitis or sepsis.
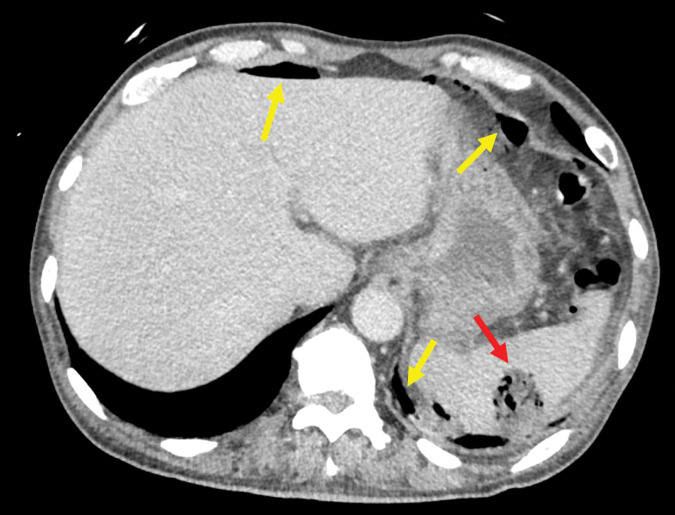
Case presentation: A 68-year-old man with uncontrolled diabetes presented with fever, chills, and abdominal pain. Initial evaluation at a previous hospital, including computed tomography (CT), suggested a lower gastrointestinal perforation, leading to his transfer to our facility. CT revealed a non-enhancing lesion with gas in the spleen and free intraperitoneal air; however, there was no clear evidence of gastrointestinal perforation. An emergency exploratory laparotomy was performed, which revealed purulent ascites and a ruptured splenic abscess without any gastrointestinal perforation. After thorough lavage to eliminate contamination, open abdominal management was initiated owing to a need for catecholamine support and an inability to completely rule out the possibility of gastrointestinal perforation. A second-look laparotomy confirmed that there was no further contamination or gastrointestinal tract perforation. Blood and abscess cultures revealed Escherichia coli, leading us to initiate targeted antibiotic therapy. The patient recovered successfully and was discharged on postoperative day 40 without any recurrence. Ruptured splenic abscess with pneumoperitoneum is rare and poses significant diagnostic challenges, particularly in patients with diabetes, owing to its clinical similarity to gastrointestinal perforation. This study highlights the utility of exploratory laparotomy and staged open abdominal management when gastrointestinal perforation cannot be ruled out.
Conclusions: Physicians should consider ruptured splenic abscesses in patients with pneumoperitoneum, particularly those with diabetes. Exploratory laparotomy with staged open abdominal management may represent an effective approach that facilitates safe monitoring and targeted treatment, thereby reducing the risk of fatal complications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


