{"title":"Effect of additional intravenous immunoglobulin for infliximab-refractory Kawasaki disease: a cohort study.","authors":"Satoki Hatano, Hiro Nakao, Hiroshi Masuda, Hiroshi Ono, Mitsuru Kubota, Akira Ishiguro","doi":"10.1186/s12969-025-01108-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Infliximab (IFX) is a reliable choice of treatment for intravenous immunoglobulin (IVIG)-resistant Kawasaki disease (KD) patients. Nationwide surveys in Japan demonstrated that additional treatment was still required for 20-30% of patients after IFX infusion. Additional IVIG was selected for 70% as the treatment for KD refractory to IFX. This study aimed to describe the therapeutic effect of IVIG after IFX for patients with KD refractory to IFX.</p><p><strong>Methods: </strong>A cohort study was conducted at a single center involving patients treated with additional IVIG for KD refractory to IFX between January 2016 and March 2023 (IVIG-after-IFX group). Additionally, KD patients resistant to the initial IVIG and who received a second IVIG in 2016 were included as a comparison group (second-IVIG group). We employed descriptive statistics and survival analysis to describe their clinical course information, including the time from initiation of the treatment to resolution of fever and the appearance of coronary artery lesions (CALs).</p><p><strong>Results: </strong>The analysis included 27 cases in the IVIG-after-IFX group. The additional IVIG-after-IFX was initiated on a median 11 days of illness (range 8-29). The median time until fever resolution was 1.0 day in the IVIG-after-IFX group and 1.0 day in the second-IVIG group (P = 0.783, HR 1.00; 95% CI 0.58-1.70). The fever resolved within 2.0 days after the initiation of the therapy in 78% (21/27) in the IVIG-after-IFX group and 68% (26/38) in the second-IVIG group. CALs were identified in 26% (7/27) before initiating IVIG-after-IFX, and 7% (2/27) showed new CALs after IVIG after IFX. Persistent CALs were observed in 19% (5/27) after 12 months after diagnosis.</p><p><strong>Conclusions: </strong>Additional IVIG for IFX-refractory KD may have a therapeutic effect comparable to that of the second IVIG for IVIG-resistant KD and be a hopeful therapeutic option for IFX-refractory KD. Treatment of IFX-refractory KD remains a challenge for us and requires further exploration, particularly regarding CAL prevention.</p>","PeriodicalId":54630,"journal":{"name":"Pediatric Rheumatology","volume":"23 1","pages":"49"},"PeriodicalIF":2.3000,"publicationDate":"2025-05-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12076848/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Rheumatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12969-025-01108-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Infliximab (IFX) is a reliable choice of treatment for intravenous immunoglobulin (IVIG)-resistant Kawasaki disease (KD) patients. Nationwide surveys in Japan demonstrated that additional treatment was still required for 20-30% of patients after IFX infusion. Additional IVIG was selected for 70% as the treatment for KD refractory to IFX. This study aimed to describe the therapeutic effect of IVIG after IFX for patients with KD refractory to IFX.
Methods: A cohort study was conducted at a single center involving patients treated with additional IVIG for KD refractory to IFX between January 2016 and March 2023 (IVIG-after-IFX group). Additionally, KD patients resistant to the initial IVIG and who received a second IVIG in 2016 were included as a comparison group (second-IVIG group). We employed descriptive statistics and survival analysis to describe their clinical course information, including the time from initiation of the treatment to resolution of fever and the appearance of coronary artery lesions (CALs).
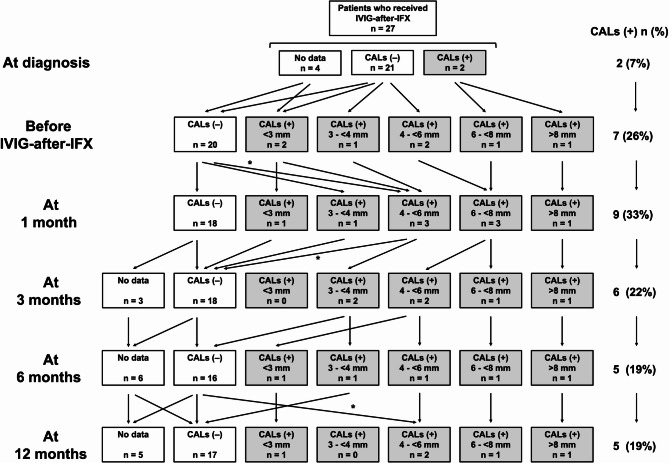
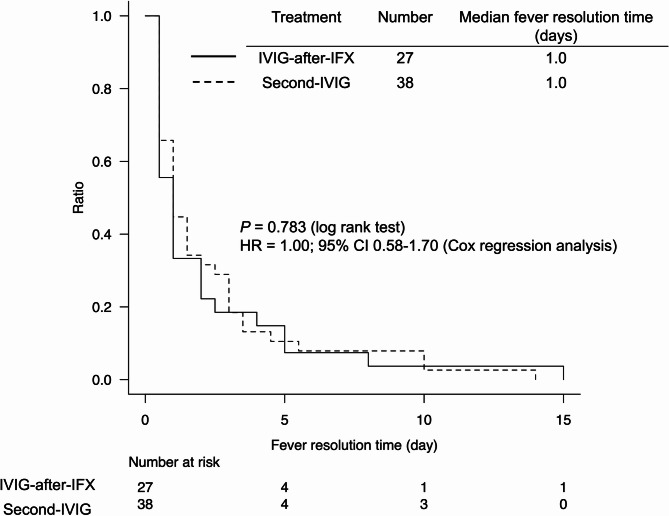
Results: The analysis included 27 cases in the IVIG-after-IFX group. The additional IVIG-after-IFX was initiated on a median 11 days of illness (range 8-29). The median time until fever resolution was 1.0 day in the IVIG-after-IFX group and 1.0 day in the second-IVIG group (P = 0.783, HR 1.00; 95% CI 0.58-1.70). The fever resolved within 2.0 days after the initiation of the therapy in 78% (21/27) in the IVIG-after-IFX group and 68% (26/38) in the second-IVIG group. CALs were identified in 26% (7/27) before initiating IVIG-after-IFX, and 7% (2/27) showed new CALs after IVIG after IFX. Persistent CALs were observed in 19% (5/27) after 12 months after diagnosis.
Conclusions: Additional IVIG for IFX-refractory KD may have a therapeutic effect comparable to that of the second IVIG for IVIG-resistant KD and be a hopeful therapeutic option for IFX-refractory KD. Treatment of IFX-refractory KD remains a challenge for us and requires further exploration, particularly regarding CAL prevention.
期刊介绍:
Pediatric Rheumatology is an open access, peer-reviewed, online journal encompassing all aspects of clinical and basic research related to pediatric rheumatology and allied subjects.
The journal’s scope of diseases and syndromes include musculoskeletal pain syndromes, rheumatic fever and post-streptococcal syndromes, juvenile idiopathic arthritis, systemic lupus erythematosus, juvenile dermatomyositis, local and systemic scleroderma, Kawasaki disease, Henoch-Schonlein purpura and other vasculitides, sarcoidosis, inherited musculoskeletal syndromes, autoinflammatory syndromes, and others.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


