James D Miller, Zachary L Mitchell, Abigail L Ellington, Felicia A Peoples, Steven B Clayton
{"title":"Functional Lumen Imaging Probe Measurement Post-Pneumatic Dilation in Clinically Relevant Esophagogastric Junction Outlet Obstruction.","authors":"James D Miller, Zachary L Mitchell, Abigail L Ellington, Felicia A Peoples, Steven B Clayton","doi":"10.1111/nmo.70053","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pneumatic dilation (PD) is an effective treatment for disorders of reduced esophageal opening. Functional lumen impedance planimetry (FLIP) can effectively measure lower esophageal sphincter (LES) physiology compared to esophageal standards. The aim of this retrospective cohort analysis was to evaluate if FLIP measurements and esophageal opening classifications changed consistently with symptom improvement post-PD. Also, the aim was to determine if post-PD FLIP measurement correlated with the need for repeat dilation.</p><p><strong>Methods: </strong>Patients with clinically significant esophagogastric junction outlet obstruction (EGJOO) with reduced esophageal opening (REO) or borderline REO (BrEO) based on FLIP, timed barium esophagram (TBE), and manometry who underwent PD were included. Post-PD FLIP measurements were taken immediately after PD during the same endoscopy encounter.</p><p><strong>Results: </strong>After PD, average distensibility index (DI) increased from 1.5 mm<sup>2</sup>/mmHg to 4.7 mm<sup>2</sup>/mmHg (p < 0.001) and diameter changed from 8.9 mm to 15.9 mm (p < 0.001). Average post-dilation Eckardt score was 1.2, decreasing from an average pre-dilation score of 6.25. Of those requiring repeat dilations, average post-dilation DI was 4.5 mm<sup>2</sup>/mmHg and diameter 16.4 mm, not statistically different from those that did not undergo repeat procedure (p = 0.79, 0.67, respectively). Post-dilation esophageal openings were all NEO or BnEO. Average Eckardt score at 6-8 week follow-up was not significantly different from those who did not require repeat dilation (1.4, p = 0.112).</p><p><strong>Conclusions: </strong>PD appears to be associated with improved esophageal opening and a significant change in both DI and diameter, consistent with an improved Eckardt score. Post-dilation DI, diameter, esophageal opening pattern, and Eckardt score did not reveal a trend indicating the need for repeat dilation.</p>","PeriodicalId":19123,"journal":{"name":"Neurogastroenterology and Motility","volume":" ","pages":"e70053"},"PeriodicalIF":2.9000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12435797/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurogastroenterology and Motility","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/nmo.70053","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/24 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Pneumatic dilation (PD) is an effective treatment for disorders of reduced esophageal opening. Functional lumen impedance planimetry (FLIP) can effectively measure lower esophageal sphincter (LES) physiology compared to esophageal standards. The aim of this retrospective cohort analysis was to evaluate if FLIP measurements and esophageal opening classifications changed consistently with symptom improvement post-PD. Also, the aim was to determine if post-PD FLIP measurement correlated with the need for repeat dilation.
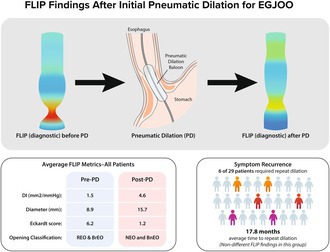
Methods: Patients with clinically significant esophagogastric junction outlet obstruction (EGJOO) with reduced esophageal opening (REO) or borderline REO (BrEO) based on FLIP, timed barium esophagram (TBE), and manometry who underwent PD were included. Post-PD FLIP measurements were taken immediately after PD during the same endoscopy encounter.
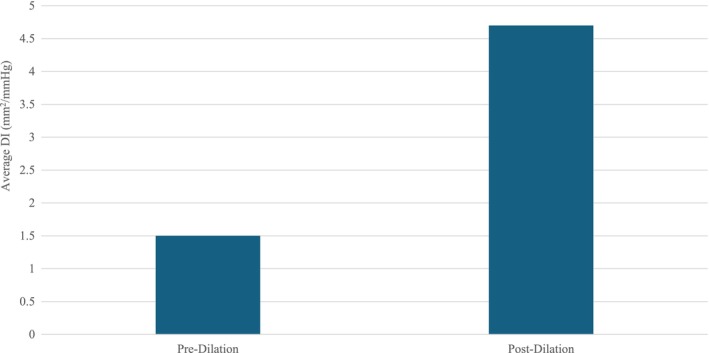
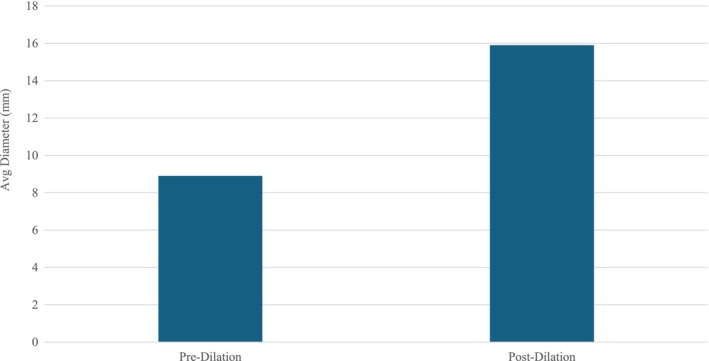
Results: After PD, average distensibility index (DI) increased from 1.5 mm2/mmHg to 4.7 mm2/mmHg (p < 0.001) and diameter changed from 8.9 mm to 15.9 mm (p < 0.001). Average post-dilation Eckardt score was 1.2, decreasing from an average pre-dilation score of 6.25. Of those requiring repeat dilations, average post-dilation DI was 4.5 mm2/mmHg and diameter 16.4 mm, not statistically different from those that did not undergo repeat procedure (p = 0.79, 0.67, respectively). Post-dilation esophageal openings were all NEO or BnEO. Average Eckardt score at 6-8 week follow-up was not significantly different from those who did not require repeat dilation (1.4, p = 0.112).
Conclusions: PD appears to be associated with improved esophageal opening and a significant change in both DI and diameter, consistent with an improved Eckardt score. Post-dilation DI, diameter, esophageal opening pattern, and Eckardt score did not reveal a trend indicating the need for repeat dilation.
期刊介绍:
Neurogastroenterology & Motility (NMO) is the official Journal of the European Society of Neurogastroenterology & Motility (ESNM) and the American Neurogastroenterology and Motility Society (ANMS). It is edited by James Galligan, Albert Bredenoord, and Stephen Vanner. The editorial and peer review process is independent of the societies affiliated to the journal and publisher: Neither the ANMS, the ESNM or the Publisher have editorial decision-making power. Whenever these are relevant to the content being considered or published, the editors, journal management committee and editorial board declare their interests and affiliations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


