Teruhisa Mihata, Masaki Akeda, Michael Künzler, Michelle H McGarry, Thay Q Lee
{"title":"Biomechanical analysis of ulnar nerve gliding and elongation: implications for nonsurgical ulnar nerve release in cubital tunnel syndrome.","authors":"Teruhisa Mihata, Masaki Akeda, Michael Künzler, Michelle H McGarry, Thay Q Lee","doi":"10.5397/cise.2024.00934","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Nonsurgical ulnar nerve release was developed for conservative treatment of cubital tunnel syndrome. Our objective in this study was to investigate the amount of ulnar nerve gliding and elongation during passive wrist, forearm, or elbow movements to determine the most effective nonsurgical ulnar nerve release technique.</p><p><strong>Methods: </strong>Seven fresh-frozen cadaveric upper limbs were tested in an elbow-testing system. Ulnar nerve gliding (mobility) and elongation (stretching) were measured around the elbow joint using a three-dimensional digitizing system. Data were compared between arm positions (elbow extension vs. 90° flexion, wrist extension vs. flexion, or forearm pronation vs. supination).</p><p><strong>Results: </strong>Passive wrist movement from flexion to extension caused the ulnar nerve to glide. The largest amount of glide during passive wrist movement was found at 90° elbow flexion and maximum forearm supination position (5.4±1.1 mm). Ulnar nerve gliding during passive forearm movement was subtle. The ulnar nerve tightened with elbow flexion. Maximum elongation of the ulnar nerve was 5.6±0.6 mm from extension to 90° flexion in the elbow.</p><p><strong>Conclusions: </strong>Ulnar nerve gliding was most severe during passive wrist movement in elbow flexion and forearm supination. This result suggests that passive wrist movement from flexion to extension with the elbow flexed and forearm supinated may be the most effective nonsurgical ulnar nerve release position to treat cubital tunnel syndrome. Attention should be paid to the elbow flexion angle during nonsurgical ulnar nerve release to not exacerbate cubital tunnel symptoms. Level of evidence: III.</p>","PeriodicalId":33981,"journal":{"name":"Clinics in Shoulder and Elbow","volume":" ","pages":"137-145"},"PeriodicalIF":1.7000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12151652/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinics in Shoulder and Elbow","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5397/cise.2024.00934","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/25 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Nonsurgical ulnar nerve release was developed for conservative treatment of cubital tunnel syndrome. Our objective in this study was to investigate the amount of ulnar nerve gliding and elongation during passive wrist, forearm, or elbow movements to determine the most effective nonsurgical ulnar nerve release technique.
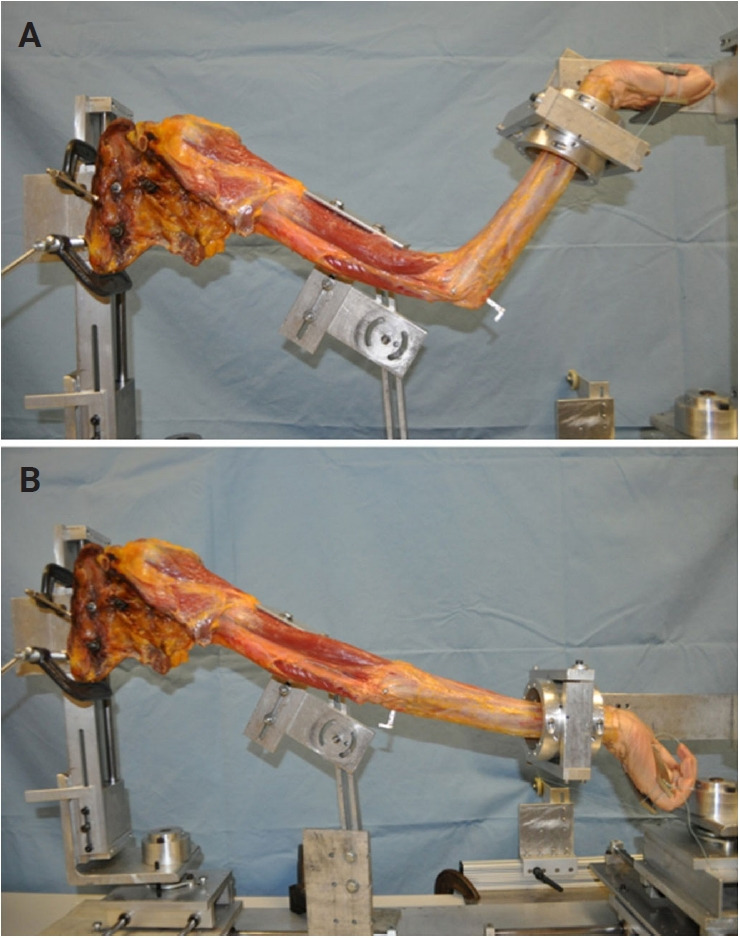
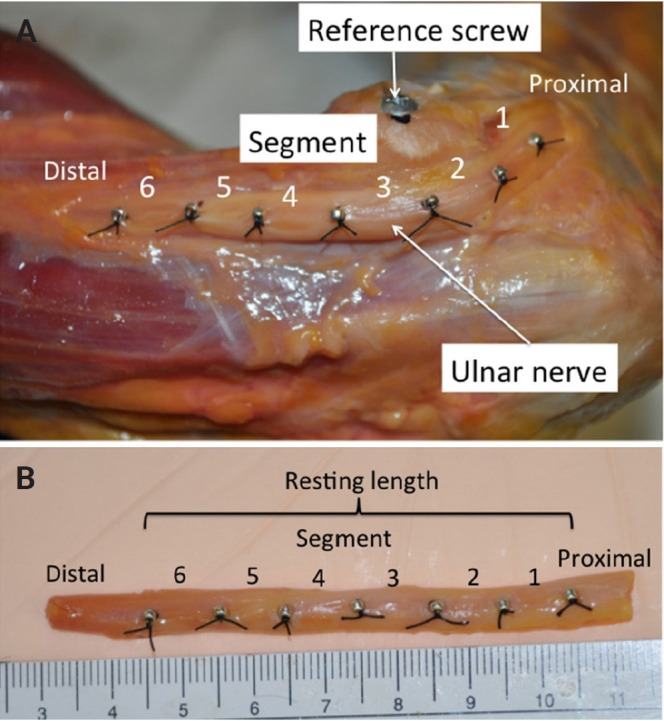
Methods: Seven fresh-frozen cadaveric upper limbs were tested in an elbow-testing system. Ulnar nerve gliding (mobility) and elongation (stretching) were measured around the elbow joint using a three-dimensional digitizing system. Data were compared between arm positions (elbow extension vs. 90° flexion, wrist extension vs. flexion, or forearm pronation vs. supination).
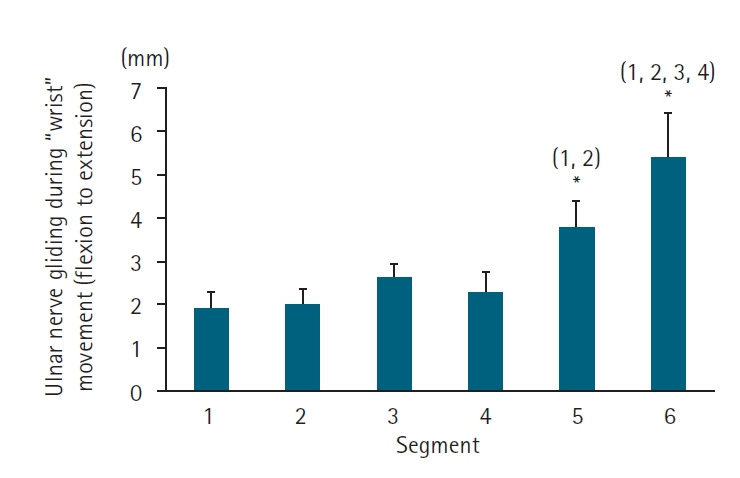
Results: Passive wrist movement from flexion to extension caused the ulnar nerve to glide. The largest amount of glide during passive wrist movement was found at 90° elbow flexion and maximum forearm supination position (5.4±1.1 mm). Ulnar nerve gliding during passive forearm movement was subtle. The ulnar nerve tightened with elbow flexion. Maximum elongation of the ulnar nerve was 5.6±0.6 mm from extension to 90° flexion in the elbow.
Conclusions: Ulnar nerve gliding was most severe during passive wrist movement in elbow flexion and forearm supination. This result suggests that passive wrist movement from flexion to extension with the elbow flexed and forearm supinated may be the most effective nonsurgical ulnar nerve release position to treat cubital tunnel syndrome. Attention should be paid to the elbow flexion angle during nonsurgical ulnar nerve release to not exacerbate cubital tunnel symptoms. Level of evidence: III.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


