Real-world data analysis of survival outcomes of patients with primary mediastinal large B-cell lymphoma treated with immunochemotherapy: the role of consolidative radiation therapy.
Yong-Pyo Lee, Junhun Cho, Young Hyeh Ko, Dongryul Oh, Seok Jin Kim, Won Seog Kim, Sang Eun Yoon
{"title":"Real-world data analysis of survival outcomes of patients with primary mediastinal large B-cell lymphoma treated with immunochemotherapy: the role of consolidative radiation therapy.","authors":"Yong-Pyo Lee, Junhun Cho, Young Hyeh Ko, Dongryul Oh, Seok Jin Kim, Won Seog Kim, Sang Eun Yoon","doi":"10.1007/s44313-025-00076-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Primary mediastinal large B-cell lymphoma (PMBCL) is a rare subtype of diffuse large B-cell lymphoma. Radiation therapy (RT) has served as the primary treatment option for PMBCL; however, its role has been questioned with the advent of intensified immunochemotherapy. This study aimed to investigate the role of consolidative RT in the primary treatment of PMBCL.</p><p><strong>Methods: </strong>This single-center retrospective study analyzed the survival outcomes of 65 patients newly diagnosed with PMBCL. The patients were divided into three treatment groups: (1) EPOCH-R (etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin, and rituximab), (2) R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone), and (3) R-CHOP with consolidative RT.</p><p><strong>Results: </strong>The objective response and complete remission rates were 86.2% and 63.1%, respectively, with 3-year progression-free survival (PFS) and overall survival (OS) rates of 72% and 81%, respectively. All patients in the R-CHOP + RT group achieved an objective response with better PFS) than those who did not receive consolidative RT (p = 0.028), although there was no significant difference in OS (p = 0.102). Consolidative RT benefited patients with an initially bulky disease or insufficient end-of-treatment response. The predictive value of <sup>18</sup>F-fluorodeoxyglucose positron-emission tomography-computed tomography (PET-CT) in assessing the treatment response in PMBCL was revalidated, showing that patients who achieved negative end-of-treatment PET-CT had significantly better survival outcomes than others.</p><p><strong>Conclusions: </strong>R-CHOP is a useful alternative regimen when intensified chemotherapy is not feasible. Consolidative RT should be considered in cases with an initially bulky disease and insufficient end-of-treatment response.</p>","PeriodicalId":46224,"journal":{"name":"Blood Research","volume":"60 1","pages":"27"},"PeriodicalIF":2.8000,"publicationDate":"2025-04-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12014970/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s44313-025-00076-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Primary mediastinal large B-cell lymphoma (PMBCL) is a rare subtype of diffuse large B-cell lymphoma. Radiation therapy (RT) has served as the primary treatment option for PMBCL; however, its role has been questioned with the advent of intensified immunochemotherapy. This study aimed to investigate the role of consolidative RT in the primary treatment of PMBCL.
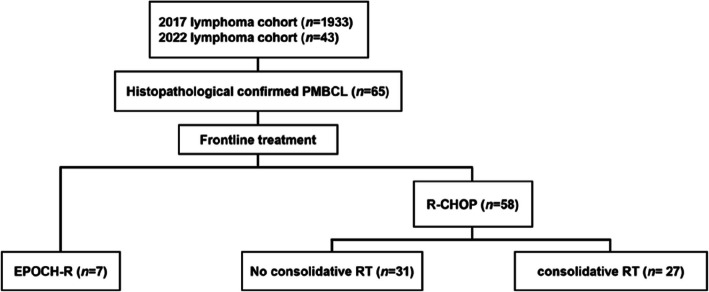
Methods: This single-center retrospective study analyzed the survival outcomes of 65 patients newly diagnosed with PMBCL. The patients were divided into three treatment groups: (1) EPOCH-R (etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin, and rituximab), (2) R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone), and (3) R-CHOP with consolidative RT.
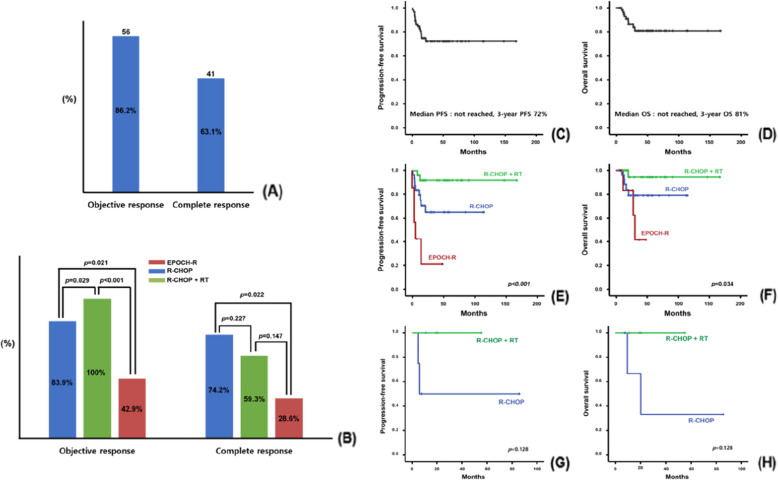
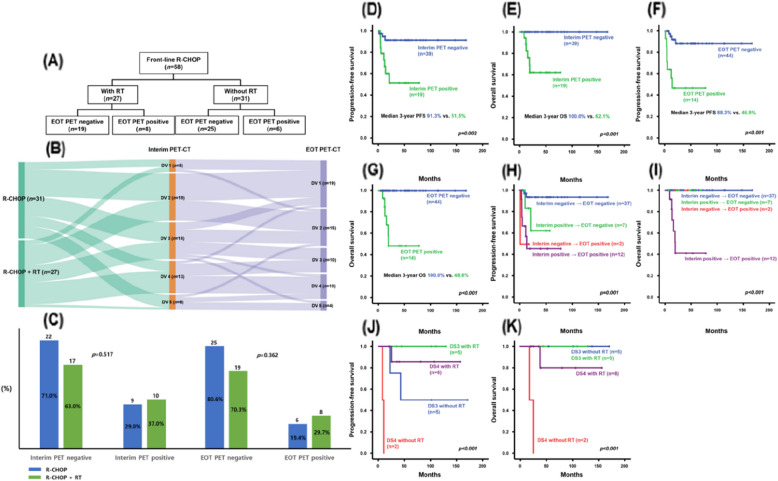
Results: The objective response and complete remission rates were 86.2% and 63.1%, respectively, with 3-year progression-free survival (PFS) and overall survival (OS) rates of 72% and 81%, respectively. All patients in the R-CHOP + RT group achieved an objective response with better PFS) than those who did not receive consolidative RT (p = 0.028), although there was no significant difference in OS (p = 0.102). Consolidative RT benefited patients with an initially bulky disease or insufficient end-of-treatment response. The predictive value of 18F-fluorodeoxyglucose positron-emission tomography-computed tomography (PET-CT) in assessing the treatment response in PMBCL was revalidated, showing that patients who achieved negative end-of-treatment PET-CT had significantly better survival outcomes than others.
Conclusions: R-CHOP is a useful alternative regimen when intensified chemotherapy is not feasible. Consolidative RT should be considered in cases with an initially bulky disease and insufficient end-of-treatment response.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


