Malik W Z Khan, Muhammad Ahmad, Salma Qudrat, Long Tu, Salman Khan, Ekrem Yetiskul, Samra Iftikhar
{"title":"Failure of the tyrosine kinase inhibitors osimertinib and erlotinib to manage a patient with EGFR-mutant lung adenocarcinoma: a case report.","authors":"Malik W Z Khan, Muhammad Ahmad, Salma Qudrat, Long Tu, Salman Khan, Ekrem Yetiskul, Samra Iftikhar","doi":"10.21037/acr-24-122","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Lung adenocarcinoma, a type of non-small cell lung cancer (NSCLC), is the most common type of lung cancer among non-smokers. Lung adenocarcinoma in exon 19 deletion (E19del) mutation-positive cases respond well to treatment with tyrosine kinase inhibitors (TKIs). Our case demonstrates the development of resistance to first- and third-generation TKIs in a 48-year-old woman with epidermal growth factor receptor (EGFR) mutation-positive advanced NSCLC.</p><p><strong>Case description: </strong>A 48 years old woman with no smoking history and no family history of cancer was diagnosed with EGFR mutation-positive advanced lung adenocarcinoma. Molecular analysis indicated a positive EGFR E19del mutation and a positive T790M mutation, and after two rounds of chemotherapy, the patient was treated with osimertinib for 2 years. However, the patient started to experience recurring chest discomfort, dyspnea, insomnia, and bone pain while being treated. A whole-body computed tomography (CT) scan at that time revealed metastasis of the tumor to the paraaortic lymph nodes and lumbar spine. A repeat analysis revealed that the T790M mutation had disappeared while other mutations remained unchanged, and she was switched to erlotinib as per the evidence for the use of erlotinib in osimertinib-resistant lung cancer. The patient developed cutaneous adverse reactions and, although her symptoms subsided initially for 6 months, she developed morning headaches and worsening insomnia. A repeat magnetic resonance imaging (MRI) revealed metastasis to the frontal and occipital lobes of her brain, indicating failure of erlotinib treatment.</p><p><strong>Conclusions: </strong>Resistance development to TKIs poses a significant challenge to the treatment of EGFR mutation-positive advanced lung adenocarcinoma, owing to the scarce availability of further pharmacological agents post-TKIs. This case illustrates the significance of prompt recognition of resistance to erlotinib and osimertinib and highlights the importance of further research to prevent treatment failure and hence, to deter metastatic progression of the tumor in patients with advanced NSCLC.</p>","PeriodicalId":29752,"journal":{"name":"AME Case Reports","volume":"9 ","pages":"53"},"PeriodicalIF":0.7000,"publicationDate":"2025-04-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12053439/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AME Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/acr-24-122","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Lung adenocarcinoma, a type of non-small cell lung cancer (NSCLC), is the most common type of lung cancer among non-smokers. Lung adenocarcinoma in exon 19 deletion (E19del) mutation-positive cases respond well to treatment with tyrosine kinase inhibitors (TKIs). Our case demonstrates the development of resistance to first- and third-generation TKIs in a 48-year-old woman with epidermal growth factor receptor (EGFR) mutation-positive advanced NSCLC.
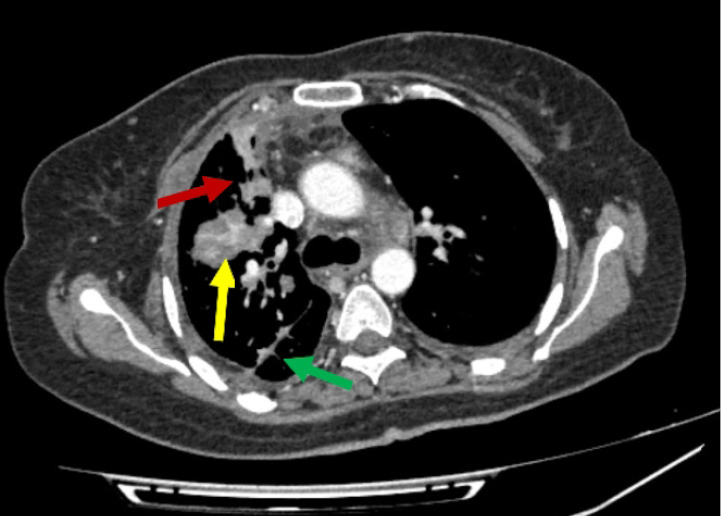
Case description: A 48 years old woman with no smoking history and no family history of cancer was diagnosed with EGFR mutation-positive advanced lung adenocarcinoma. Molecular analysis indicated a positive EGFR E19del mutation and a positive T790M mutation, and after two rounds of chemotherapy, the patient was treated with osimertinib for 2 years. However, the patient started to experience recurring chest discomfort, dyspnea, insomnia, and bone pain while being treated. A whole-body computed tomography (CT) scan at that time revealed metastasis of the tumor to the paraaortic lymph nodes and lumbar spine. A repeat analysis revealed that the T790M mutation had disappeared while other mutations remained unchanged, and she was switched to erlotinib as per the evidence for the use of erlotinib in osimertinib-resistant lung cancer. The patient developed cutaneous adverse reactions and, although her symptoms subsided initially for 6 months, she developed morning headaches and worsening insomnia. A repeat magnetic resonance imaging (MRI) revealed metastasis to the frontal and occipital lobes of her brain, indicating failure of erlotinib treatment.
Conclusions: Resistance development to TKIs poses a significant challenge to the treatment of EGFR mutation-positive advanced lung adenocarcinoma, owing to the scarce availability of further pharmacological agents post-TKIs. This case illustrates the significance of prompt recognition of resistance to erlotinib and osimertinib and highlights the importance of further research to prevent treatment failure and hence, to deter metastatic progression of the tumor in patients with advanced NSCLC.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


