{"title":"Mortality predictors and diagnostic challenges in adult tuberculous meningitis: a retrospective cohort of 100 patients.","authors":"Mahboubeh Maleki Rad, Mahboubeh Haddad, Fereshte Sheybani, Matin Shirazinia, Maliheh Dadgarmoghaddam","doi":"10.1186/s41182-025-00738-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study aimed to assess the clinical characteristics, diagnostic certainty, outcomes, and predictors of mortality in patients diagnosed with tuberculous meningitis (TBM), using the Lancet scoring system for diagnostic certainty.</p><p><strong>Methods: </strong>A retrospective cohort was conducted on 100 patients diagnosed with TBM. Patients were classified based on the Lancet scoring system into definite, probable, and possible TBM categories. Clinical features, neuroimaging findings, cerebrospinal fluid (CSF) analysis, and outcomes were analyzed.</p><p><strong>Results: </strong>The median age of patients was 36.5 years, with 57.0% male. The most common symptoms were fever (64.7%), headache (63.6%), and altered consciousness (60.0%). Hydrocephalus was present in 40.0% of cases. Diagnosis certainty was classified as possible (63.0%), probable (22.0%), and definite (15.0%). The in-hospital mortality rate was 18.0%, with 12-month survival rates of 69.7%. There was no significant difference between the level of diagnostic certainty and the survival of patients. Significant predictors of mortality included hydrocephalus (hazard ratio [HR]: 3.65, 95% CI 1.67 to 7.97), hemoglobin levels (HR: 0.75, 95% CI 0.64 to 0.89), age (HR: 1.04, 95% CI 1.02 to 1.06), CSF pleocytosis (HR: 0.34, 95% CI 0.14 to 0.84), and altered consciousness at admission (HR: 19.23, 95% CI 2.57 to 143.85).</p><p><strong>Conclusion: </strong>TBM remains a critical concern with significant mortality and morbidity. Key predictors of mortality, including altered consciousness, hydrocephalus, and older age, highlight the need for early detection and tailored interventions. In most cases, the diagnosis cannot be definitively confirmed and is instead categorized as probable or possible. Our study demonstrates that survival rates were comparable across definite, probable, and possible TBM categories, supporting the value of empirical treatment when definitive confirmation is not feasible.</p>","PeriodicalId":23311,"journal":{"name":"Tropical Medicine and Health","volume":"53 1","pages":"58"},"PeriodicalIF":3.5000,"publicationDate":"2025-04-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12020108/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Tropical Medicine and Health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41182-025-00738-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"TROPICAL MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: This study aimed to assess the clinical characteristics, diagnostic certainty, outcomes, and predictors of mortality in patients diagnosed with tuberculous meningitis (TBM), using the Lancet scoring system for diagnostic certainty.
Methods: A retrospective cohort was conducted on 100 patients diagnosed with TBM. Patients were classified based on the Lancet scoring system into definite, probable, and possible TBM categories. Clinical features, neuroimaging findings, cerebrospinal fluid (CSF) analysis, and outcomes were analyzed.
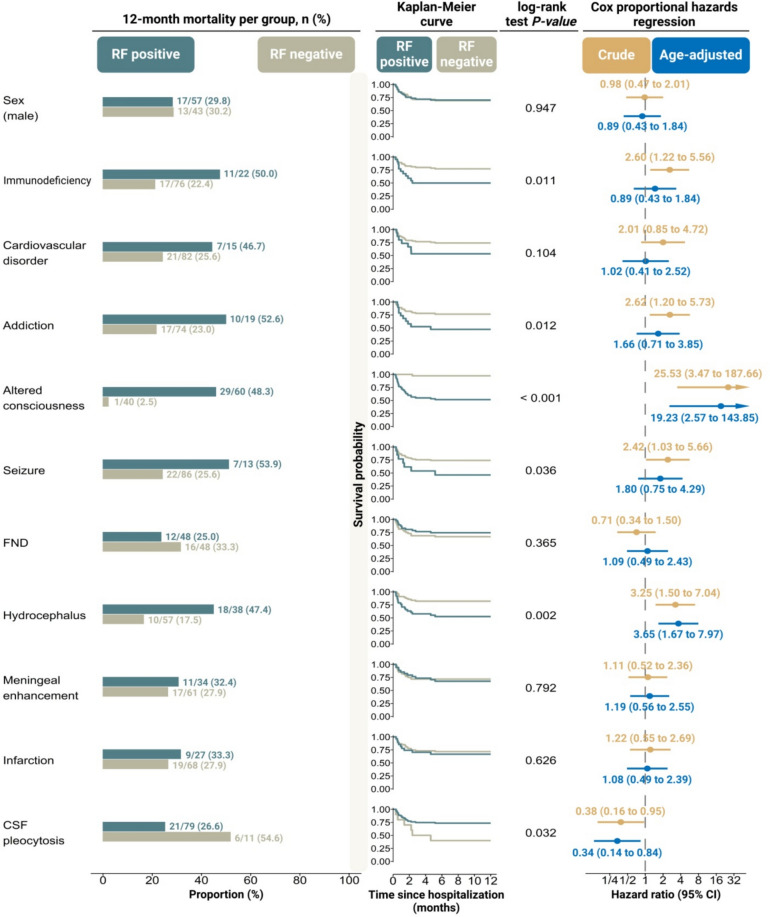
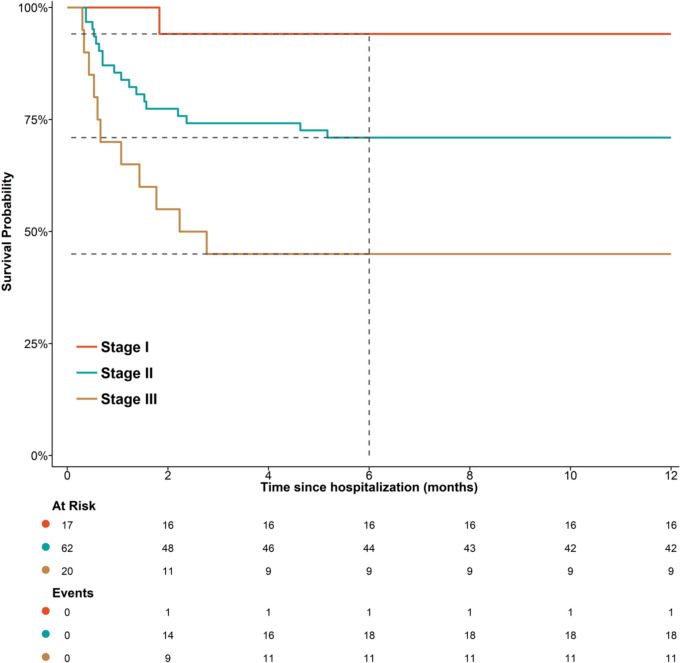
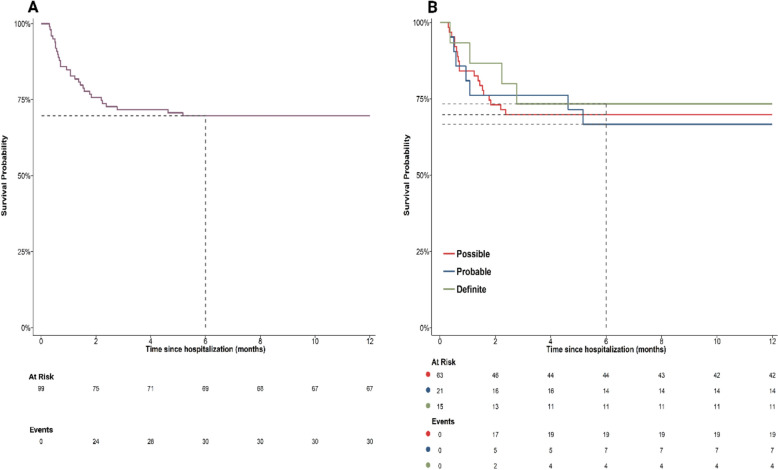
Results: The median age of patients was 36.5 years, with 57.0% male. The most common symptoms were fever (64.7%), headache (63.6%), and altered consciousness (60.0%). Hydrocephalus was present in 40.0% of cases. Diagnosis certainty was classified as possible (63.0%), probable (22.0%), and definite (15.0%). The in-hospital mortality rate was 18.0%, with 12-month survival rates of 69.7%. There was no significant difference between the level of diagnostic certainty and the survival of patients. Significant predictors of mortality included hydrocephalus (hazard ratio [HR]: 3.65, 95% CI 1.67 to 7.97), hemoglobin levels (HR: 0.75, 95% CI 0.64 to 0.89), age (HR: 1.04, 95% CI 1.02 to 1.06), CSF pleocytosis (HR: 0.34, 95% CI 0.14 to 0.84), and altered consciousness at admission (HR: 19.23, 95% CI 2.57 to 143.85).
Conclusion: TBM remains a critical concern with significant mortality and morbidity. Key predictors of mortality, including altered consciousness, hydrocephalus, and older age, highlight the need for early detection and tailored interventions. In most cases, the diagnosis cannot be definitively confirmed and is instead categorized as probable or possible. Our study demonstrates that survival rates were comparable across definite, probable, and possible TBM categories, supporting the value of empirical treatment when definitive confirmation is not feasible.
目的:本研究旨在评估结核性脑膜炎(TBM)患者的临床特征、诊断确定性、结局和死亡率预测因素,采用《柳叶刀》诊断确定性评分系统。方法:对100例确诊为TBM的患者进行回顾性队列分析。根据《柳叶刀》评分系统将患者分为明确、可能和可能的TBM类别。分析临床特征、神经影像学表现、脑脊液(CSF)分析和结果。结果:患者中位年龄36.5岁,男性占57.0%。最常见的症状是发热(64.7%)、头痛(63.6%)和意识改变(60.0%)。40.0%的病例存在脑积水。诊断确定性分为可能(63.0%)、可能(22.0%)和明确(15.0%)。住院死亡率为18.0%,12个月生存率为69.7%。诊断确定性水平与患者生存率之间无显著差异。死亡率的重要预测因素包括脑积水(危险比[HR]: 3.65, 95% CI 1.67 ~ 7.97)、血红蛋白水平(危险比[HR]: 0.75, 95% CI 0.64 ~ 0.89)、年龄(危险比:1.04,95% CI 1.02 ~ 1.06)、脑脊液多细胞症(危险比:0.34,95% CI 0.14 ~ 0.84)和入院时意识改变(危险比:19.23,95% CI 2.57 ~ 143.85)。结论:TBM仍然是一个严重的问题,具有显著的死亡率和发病率。死亡率的主要预测因素,包括意识改变、脑积水和年龄增大,强调了早期发现和有针对性干预的必要性。在大多数情况下,诊断不能明确确认,而被归类为可能或可能。我们的研究表明,在确定的、可能的和可能的TBM类别中,生存率具有可比性,这支持了在无法进行明确确认时经验治疗的价值。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


