{"title":"Postoperative Intra-Pouch Mucosal Bridge Formation in a Child with Ulcerative Colitis.","authors":"Yuhki Koike, Koki Higashi, Yuki Sato, Shinji Yamashita, Yuka Nagano, Tadanobu Shimura, Takahito Kitajima, Kohei Matsushita, Yoshinaga Okugawa, Yoshiki Okita, Yuji Toiyama","doi":"10.70352/scrj.cr.25-0045","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Restorative proctocolectomy with construction of an ileal J-pouch anal anastomosis is an established gold standard procedure for managing ulcerative colitis. One of the reported complications is a residual mucosal bridge as a result of leaving an apical bridge remnant when constructing the ileal J-pouch. However, now that the surgical procedure is well established, such complications rarely occur.</p><p><strong>Case presentation: </strong>A 12-year-old girl presented to our hospital because of anal pain. She had undergone three-stage surgery for ulcerative colitis refractory to medical therapy, the third stage (stoma closure) having been performed 1 month before the present admission. A computed tomography scan to investigate the possibility of a perianal or pelvic abscess showed no abscess, but revealed what appeared to be a thickening of the wall of the J-pouch, suggestive of pouchitis. Endoscopy revealed a mucosal bridge crossing the anterior and posterior walls of the J-pouch, with a stapler line near the posterior wall's root; however, there was no evidence of pouchitis. While creating the J-pouch (during the second stage of surgery for ulcerative colitis), we had ensured that an apical bridge was eliminated with a linear stapler. Moreover, a contrast enema of the J-pouch during the present admission demonstrated interruption of contrast in the J-pouch. These findings led us to conclude that the mucosal bridge had probably formed postoperatively, after J-pouch creation. The patient underwent endoscopic resection of the mucosal bridge in the J-pouch using an XXS wound retractor transanally. Both ends of the bridge were cut three times with a 5-mm stapler and the bridge was resected. The patient was discharged after surgery, having experienced immediate resolution of anal pain and no complications. Pathological examination of the resected specimen showed that the ileal wall had bent toward the J-pouch lumen with fibrous adherence on the serosal side, indicating that the mucosal bridge had developed unintentionally post-stoma closure. Preoperative computed tomography showed limited pouch expansion, whereas postoperative computed tomography showed sufficient expansion.</p><p><strong>Conclusion: </strong>If anal pain develops following radical ulcerative colitis surgery (after ileal stoma closure), postoperative mucosal bridge formation should be included in the differential diagnosis.</p>","PeriodicalId":22096,"journal":{"name":"Surgical Case Reports","volume":"11 1","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12055236/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.70352/scrj.cr.25-0045","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/2 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Restorative proctocolectomy with construction of an ileal J-pouch anal anastomosis is an established gold standard procedure for managing ulcerative colitis. One of the reported complications is a residual mucosal bridge as a result of leaving an apical bridge remnant when constructing the ileal J-pouch. However, now that the surgical procedure is well established, such complications rarely occur.
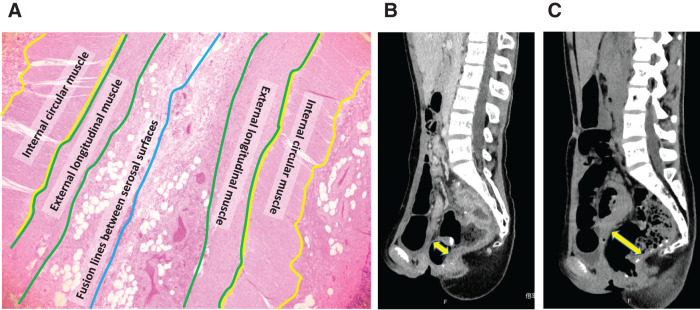
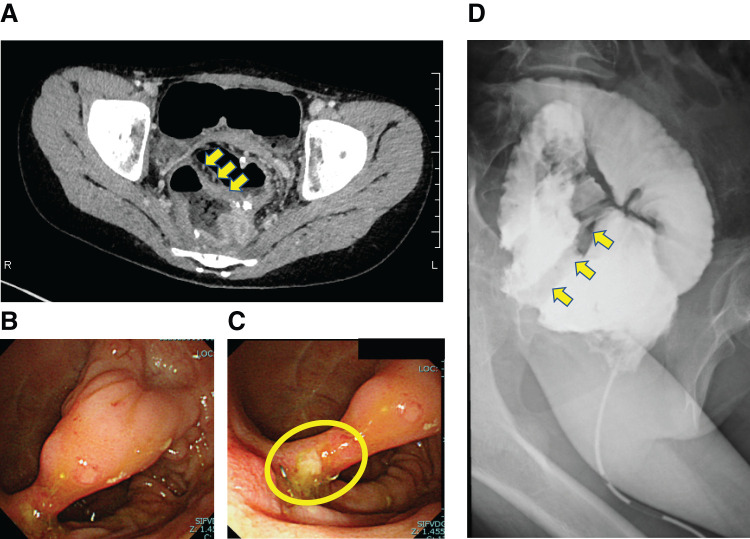
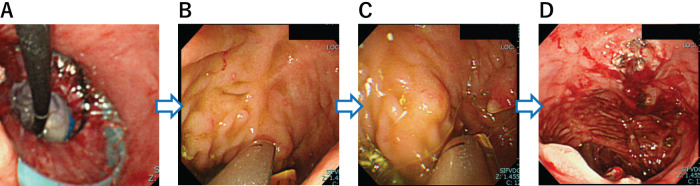
Case presentation: A 12-year-old girl presented to our hospital because of anal pain. She had undergone three-stage surgery for ulcerative colitis refractory to medical therapy, the third stage (stoma closure) having been performed 1 month before the present admission. A computed tomography scan to investigate the possibility of a perianal or pelvic abscess showed no abscess, but revealed what appeared to be a thickening of the wall of the J-pouch, suggestive of pouchitis. Endoscopy revealed a mucosal bridge crossing the anterior and posterior walls of the J-pouch, with a stapler line near the posterior wall's root; however, there was no evidence of pouchitis. While creating the J-pouch (during the second stage of surgery for ulcerative colitis), we had ensured that an apical bridge was eliminated with a linear stapler. Moreover, a contrast enema of the J-pouch during the present admission demonstrated interruption of contrast in the J-pouch. These findings led us to conclude that the mucosal bridge had probably formed postoperatively, after J-pouch creation. The patient underwent endoscopic resection of the mucosal bridge in the J-pouch using an XXS wound retractor transanally. Both ends of the bridge were cut three times with a 5-mm stapler and the bridge was resected. The patient was discharged after surgery, having experienced immediate resolution of anal pain and no complications. Pathological examination of the resected specimen showed that the ileal wall had bent toward the J-pouch lumen with fibrous adherence on the serosal side, indicating that the mucosal bridge had developed unintentionally post-stoma closure. Preoperative computed tomography showed limited pouch expansion, whereas postoperative computed tomography showed sufficient expansion.
Conclusion: If anal pain develops following radical ulcerative colitis surgery (after ileal stoma closure), postoperative mucosal bridge formation should be included in the differential diagnosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


