{"title":"Pediatric posttraumatic macular rupture.","authors":"Hasimbegovic Selma, Stojanovic Andjela, Peric Miroslav, Tomic Zoran, Pidro Miokovic Ajla, Pidro Gadzo Aida","doi":"10.22336/rjo.2025.21","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Macular rupture following ocular trauma is an uncommon but significant complication that can lead to vision loss. Due to the scarcity of literature on treatment options for traumatic macular ruptures (TMR) in pediatric patients, this case report aims to provide scientific insight and share our positive experience in treating a pediatric TMR.</p><p><strong>Materials and methods: </strong>A 6-year-old patient presented with reduced vision in the right eye following blunt trauma. Initial examination revealed hyphema, corneal edema, post-traumatic uveitis, and diminished visual acuity. Despite improvement in anterior segment findings, OCT confirmed a persistent full-thickness macular rupture three months post-injury, prompting surgical intervention.</p><p><strong>Results: </strong>After three months of observation to allow spontaneous closure, the patient underwent pars plana vitrectomy (PPV) with internal limiting membrane (ILM) peeling using the inverted flap technique and SF6 gas tamponade. OCT showed a closed macular rupture three months after surgery with residual tissue reorganization, and visual acuity improved from 0.02 to 0.3. The surgical approach resulted in successful anatomical closure and moderate functional improvement.</p><p><strong>Discussion: </strong>This case report highlights the successful management of a pediatric traumatic macular rupture (TMR) using pars plana vitrectomy (PPV) with internal limiting membrane (ILM) peeling. Despite the limited literature on the optimal treatment for TMR in children, the surgical approach described resulted in anatomic closure and functional improvement in the patient. The report emphasizes the importance of individualized treatment, considering both conservative and surgical options, particularly in cases where spontaneous closure is unlikely or delayed.</p><p><strong>Conclusion: </strong>TMH management in pediatric patients poses unique challenges due to a lack of standardized treatment protocols. While conservative observation is acceptable in cases with a higher chance of spontaneous closure, surgical intervention should be considered for more significant or persistent ruptures.</p>","PeriodicalId":94355,"journal":{"name":"Romanian journal of ophthalmology","volume":"69 1","pages":"129-133"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12049662/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Romanian journal of ophthalmology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22336/rjo.2025.21","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Macular rupture following ocular trauma is an uncommon but significant complication that can lead to vision loss. Due to the scarcity of literature on treatment options for traumatic macular ruptures (TMR) in pediatric patients, this case report aims to provide scientific insight and share our positive experience in treating a pediatric TMR.
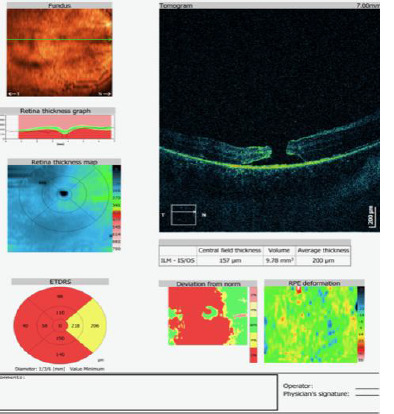
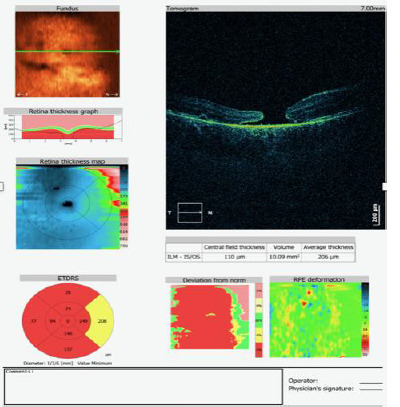
Materials and methods: A 6-year-old patient presented with reduced vision in the right eye following blunt trauma. Initial examination revealed hyphema, corneal edema, post-traumatic uveitis, and diminished visual acuity. Despite improvement in anterior segment findings, OCT confirmed a persistent full-thickness macular rupture three months post-injury, prompting surgical intervention.
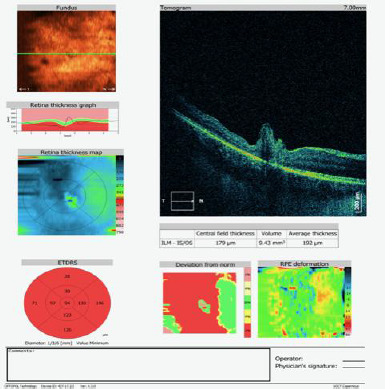
Results: After three months of observation to allow spontaneous closure, the patient underwent pars plana vitrectomy (PPV) with internal limiting membrane (ILM) peeling using the inverted flap technique and SF6 gas tamponade. OCT showed a closed macular rupture three months after surgery with residual tissue reorganization, and visual acuity improved from 0.02 to 0.3. The surgical approach resulted in successful anatomical closure and moderate functional improvement.
Discussion: This case report highlights the successful management of a pediatric traumatic macular rupture (TMR) using pars plana vitrectomy (PPV) with internal limiting membrane (ILM) peeling. Despite the limited literature on the optimal treatment for TMR in children, the surgical approach described resulted in anatomic closure and functional improvement in the patient. The report emphasizes the importance of individualized treatment, considering both conservative and surgical options, particularly in cases where spontaneous closure is unlikely or delayed.
Conclusion: TMH management in pediatric patients poses unique challenges due to a lack of standardized treatment protocols. While conservative observation is acceptable in cases with a higher chance of spontaneous closure, surgical intervention should be considered for more significant or persistent ruptures.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


