Síofra Harrington, Michael Moore, James Loughman, Ian Flitcroft, Veronica O'Dwyer
{"title":"Optimising non-cycloplegic screening strategies for early detection of pre-myopia and myopia in young children.","authors":"Síofra Harrington, Michael Moore, James Loughman, Ian Flitcroft, Veronica O'Dwyer","doi":"10.1111/opo.13525","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Early detection of myopia is essential to delay its onset and progression. Pre-myopia, defined by an inadequate hyperopic reserve, increases myopia risk in childhood. However, effective screening methods remain limited. This study aimed to develop practical non-cycloplegic screening methods for pre-myopia and myopia in 6- to 7-year-olds to support earlier interventions.</p><p><strong>Methods: </strong>This cross-sectional study of 621 Irish schoolchildren (mean age: 7.12 ± 0.45 years; 51.8% boys) assessed uncorrected distance visual acuity (UDVA). Cycloplegic spherical equivalent refraction (SER) classified refractive status (myopia: SER ≤ -0.50D; pre-myopia: SER > -0.50 ≤ 0.75D). Pre- and post-cycloplegic SER were measured using the Welch Allyn Spot Vision Screener and Dong-Yang Rekto-ORK 11, respectively. Axial length (AL) and corneal radius (CR) were measured with the Zeiss IOLMaster and parental myopia history via questionnaire. Logistic regression and ROC curves evaluated non-cycloplegic screening methods.</p><p><strong>Results: </strong>Pre-myopia prevalence was 24.3% (95% confidence intervals (CI): 29.3-36.2), and myopia prevalence was 3.3% (CI: 2.5-5.5). UDVA screening had an area under the curve (AUC) (CI) = 0.72 (0.59-0.86) and 0.42 (0.36-0.47) for detecting myopia and pre-myopia, respectively. For pre-myopia discrimination, non-cycloplegic SER, AL, AL/CR and parental myopia had AUCs of 0.67 (0.62-0.72), 0.67 (0.62-0.72), 0.69 (0.64-0.74) and 0.59 (0.53-0.64), respectively. The best method combined non-cycloplegic SER and AL/CR (AUC = 0.72 (0.67-0.76)). Including UDVA or parental myopia did not improve results. For myopia detection, AUCs were non-cycloplegic SER:0.84 (0.72-0.97), AL:0.88 (0.82-0.95), AL/CR:0.84 (0.75-0.94) and parental myopia:0.62 (0.48-0.75). The best method combined AL and non-cycloplegic SER 0.94 (0.90-0.99). Adding parental myopia did not improve the AUC = 0.93 (0.87-0.99) but adding UDVA achieved an AUC = 0.95 (0.90-0.99).</p><p><strong>Conclusion: </strong>While UDVA alone provided acceptable discrimination for myopia, it was insufficient for screening pre-myopia. Non-cycloplegic SER alone had relatively poor discrimination for pre-myopia, but its performance improved when combined with the AL/CR ratio. The best results for myopia discrimination were achieved by combining non-cycloplegic SER, axial length and UDVA measures.</p>","PeriodicalId":19522,"journal":{"name":"Ophthalmic and Physiological Optics","volume":" ","pages":"1080-1089"},"PeriodicalIF":2.4000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12153036/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ophthalmic and Physiological Optics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/opo.13525","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/14 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"OPHTHALMOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Early detection of myopia is essential to delay its onset and progression. Pre-myopia, defined by an inadequate hyperopic reserve, increases myopia risk in childhood. However, effective screening methods remain limited. This study aimed to develop practical non-cycloplegic screening methods for pre-myopia and myopia in 6- to 7-year-olds to support earlier interventions.
Methods: This cross-sectional study of 621 Irish schoolchildren (mean age: 7.12 ± 0.45 years; 51.8% boys) assessed uncorrected distance visual acuity (UDVA). Cycloplegic spherical equivalent refraction (SER) classified refractive status (myopia: SER ≤ -0.50D; pre-myopia: SER > -0.50 ≤ 0.75D). Pre- and post-cycloplegic SER were measured using the Welch Allyn Spot Vision Screener and Dong-Yang Rekto-ORK 11, respectively. Axial length (AL) and corneal radius (CR) were measured with the Zeiss IOLMaster and parental myopia history via questionnaire. Logistic regression and ROC curves evaluated non-cycloplegic screening methods.
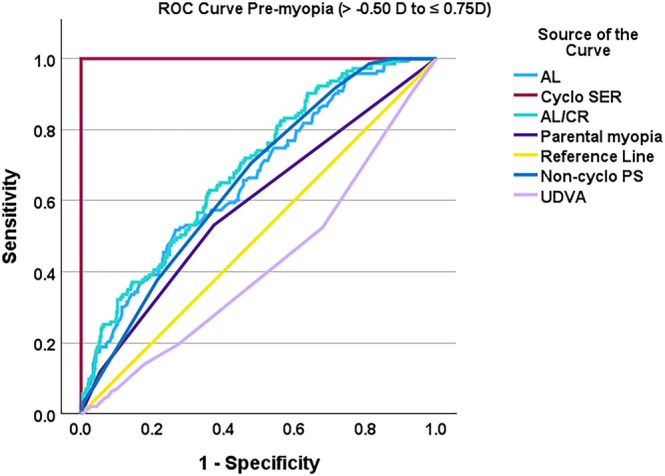
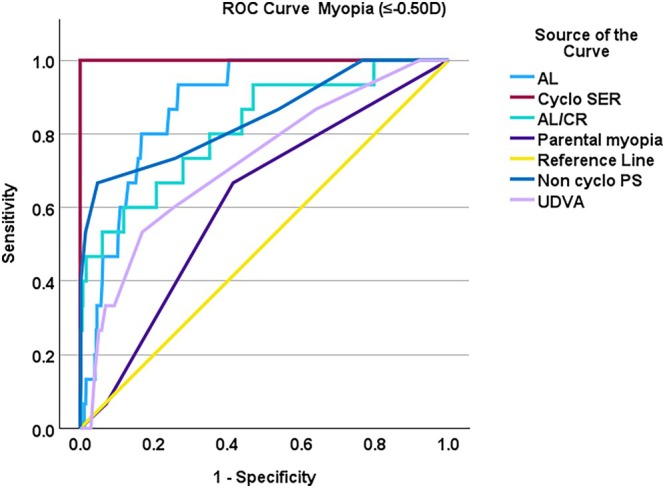
Results: Pre-myopia prevalence was 24.3% (95% confidence intervals (CI): 29.3-36.2), and myopia prevalence was 3.3% (CI: 2.5-5.5). UDVA screening had an area under the curve (AUC) (CI) = 0.72 (0.59-0.86) and 0.42 (0.36-0.47) for detecting myopia and pre-myopia, respectively. For pre-myopia discrimination, non-cycloplegic SER, AL, AL/CR and parental myopia had AUCs of 0.67 (0.62-0.72), 0.67 (0.62-0.72), 0.69 (0.64-0.74) and 0.59 (0.53-0.64), respectively. The best method combined non-cycloplegic SER and AL/CR (AUC = 0.72 (0.67-0.76)). Including UDVA or parental myopia did not improve results. For myopia detection, AUCs were non-cycloplegic SER:0.84 (0.72-0.97), AL:0.88 (0.82-0.95), AL/CR:0.84 (0.75-0.94) and parental myopia:0.62 (0.48-0.75). The best method combined AL and non-cycloplegic SER 0.94 (0.90-0.99). Adding parental myopia did not improve the AUC = 0.93 (0.87-0.99) but adding UDVA achieved an AUC = 0.95 (0.90-0.99).
Conclusion: While UDVA alone provided acceptable discrimination for myopia, it was insufficient for screening pre-myopia. Non-cycloplegic SER alone had relatively poor discrimination for pre-myopia, but its performance improved when combined with the AL/CR ratio. The best results for myopia discrimination were achieved by combining non-cycloplegic SER, axial length and UDVA measures.
期刊介绍:
Ophthalmic & Physiological Optics, first published in 1925, is a leading international interdisciplinary journal that addresses basic and applied questions pertinent to contemporary research in vision science and optometry.
OPO publishes original research papers, technical notes, reviews and letters and will interest researchers, educators and clinicians concerned with the development, use and restoration of vision.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


