Mohammad Daher, Tarishi Parmar, Peter Boufadel, Mohamad Y Fares, Wissam Khalil, John G Horneff, Joseph A Abboud, Adam Z Khan
{"title":"Patient-specific instrumentation in primary total shoulder arthroplasty: a meta-analysis of clinical outcomes.","authors":"Mohammad Daher, Tarishi Parmar, Peter Boufadel, Mohamad Y Fares, Wissam Khalil, John G Horneff, Joseph A Abboud, Adam Z Khan","doi":"10.5397/cise.2024.01095","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The introduction of patient-specific instrumentation (PSI) in total shoulder arthroplasty (TSA) has improved implant positioning accuracy. However, whether PSI yields additional clinical benefit compared to standard instrumentation (SI) in the setting of primary TSA (anatomic and reverse) remains unclear.</p><p><strong>Methods: </strong>PubMed, Cochrane, Embase, and Google Scholar were queried through August 2024. Inclusion criteria consisted of studies that compared PSI to SI in TSA (anatomic and reverse). Key outcomes analyzed included adverse events, patient-reported outcomes, and discrepancies between planned and achieved implant positioning.</p><p><strong>Results: </strong>Five retrospective studies, three randomized controlled trials, and one prospective study met the inclusion criteria. There was no difference in complications (odds ratio [OR], 1.00; 95% CI, 0.16 to 6.10; P=1.00), reoperation (OR, 1.35; 95% CI, 0.37 to 4.91; P=0.65), American Shoulder and Elbow Surgeons score (mean difference [MD], 1.61; 95% CI, -4.08 to 7.30; P=0.58), Constant-Murley Score (MD, 3.06; 95% CI, -3.68 to 9.81; P=0.37), version error (MD, -0.76; 95% CI, -2.51 to 0.99; P=0.40), and inclination error (MD, -2.89; 95% CI, -5.82 to 0.05; P=0.05) between the two groups.</p><p><strong>Conclusions: </strong>This study found no significant differences in patient-reported outcomes, complication rates, or implant positioning accuracy between PSI and SI in primary TSA. Future randomized controlled trials comparing these two types of instrumentation would be useful to assess whether a benefit exists for PSI in the setting of primary TSA. Level of evidence: III.</p>","PeriodicalId":33981,"journal":{"name":"Clinics in Shoulder and Elbow","volume":" ","pages":"129-136"},"PeriodicalIF":1.7000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12151651/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinics in Shoulder and Elbow","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5397/cise.2024.01095","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/30 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The introduction of patient-specific instrumentation (PSI) in total shoulder arthroplasty (TSA) has improved implant positioning accuracy. However, whether PSI yields additional clinical benefit compared to standard instrumentation (SI) in the setting of primary TSA (anatomic and reverse) remains unclear.
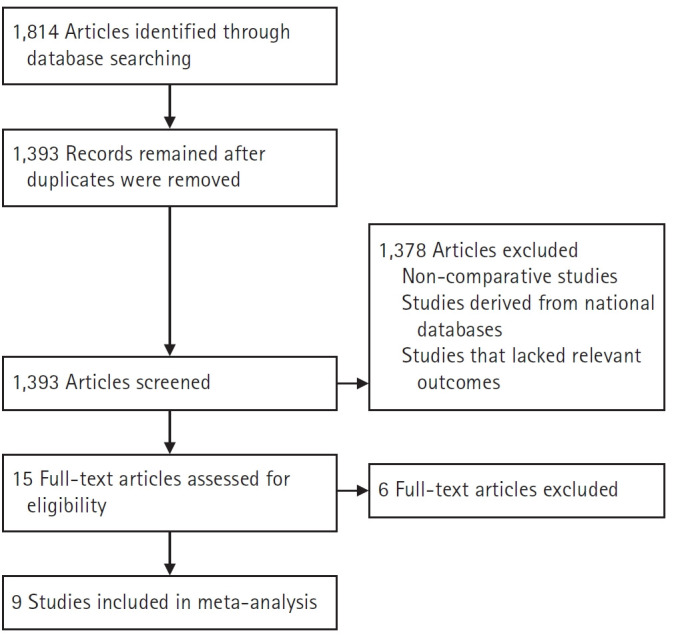
Methods: PubMed, Cochrane, Embase, and Google Scholar were queried through August 2024. Inclusion criteria consisted of studies that compared PSI to SI in TSA (anatomic and reverse). Key outcomes analyzed included adverse events, patient-reported outcomes, and discrepancies between planned and achieved implant positioning.
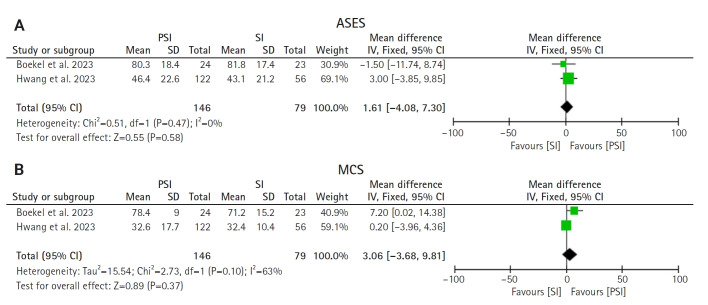
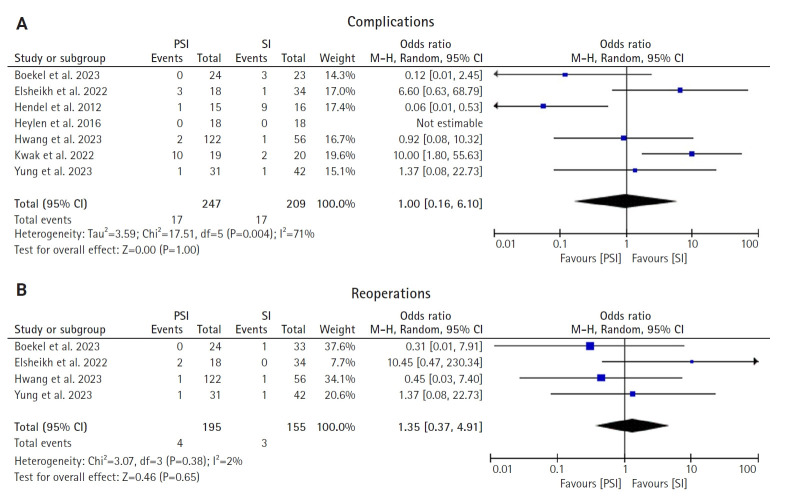
Results: Five retrospective studies, three randomized controlled trials, and one prospective study met the inclusion criteria. There was no difference in complications (odds ratio [OR], 1.00; 95% CI, 0.16 to 6.10; P=1.00), reoperation (OR, 1.35; 95% CI, 0.37 to 4.91; P=0.65), American Shoulder and Elbow Surgeons score (mean difference [MD], 1.61; 95% CI, -4.08 to 7.30; P=0.58), Constant-Murley Score (MD, 3.06; 95% CI, -3.68 to 9.81; P=0.37), version error (MD, -0.76; 95% CI, -2.51 to 0.99; P=0.40), and inclination error (MD, -2.89; 95% CI, -5.82 to 0.05; P=0.05) between the two groups.
Conclusions: This study found no significant differences in patient-reported outcomes, complication rates, or implant positioning accuracy between PSI and SI in primary TSA. Future randomized controlled trials comparing these two types of instrumentation would be useful to assess whether a benefit exists for PSI in the setting of primary TSA. Level of evidence: III.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


