Effect of pressure-controlled ventilation and volume-controlled ventilation for laparoscopic surgery in the Trendelenburg position: a systematic review and meta-analysis.
Cui Wen, Yi Qi, Yingying Xiang, Qianyun Pang, Jingyu Xiao, Ran An
{"title":"Effect of pressure-controlled ventilation and volume-controlled ventilation for laparoscopic surgery in the Trendelenburg position: a systematic review and meta-analysis.","authors":"Cui Wen, Yi Qi, Yingying Xiang, Qianyun Pang, Jingyu Xiao, Ran An","doi":"10.1186/s13741-025-00540-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Volume-controlled ventilation (VCV) and pressure-controlled ventilation (PCV) are commonly used in laparoscopic surgery in the Trendelenburg position, and pressure-controlled ventilation volume guaranteed (PCV-VG) has been increasingly used recently. However, there is still no consensus on the optimal ventilation mode. Therefore, a systematic review and meta-analysis were conducted to compare the effects of different ventilation modes for laparoscopic surgery in the Trendelenburg position.</p><p><strong>Methods: </strong>Multiple databases were searched for randomized controlled trials published before December 2024 to compare the effects of PCV, PCV-VG, and VCV in patients in the Trendelenburg position who underwent laparoscopic surgery. The primary outcomes included peak airway pressure (Ppeak), plateau airway pressure (Pplat), dynamic compliance (Cdyn), and blood gas analysis.</p><p><strong>Results: </strong>Sixteen studies were included in this meta-analysis. PCV [Ppeak, 15‒40-min post-pneumoperitoneum and Trendelenburg position (T2): mean difference (MD) - 4.28, 95% confidence interval (CI) - 5.91 to - 2.64, P < 0.01; 60-min post-pneumoperitoneum and Trendelenburg position (T3): MD - 4.51, 95% CI - 5.41 to - 3.6, P < 0.01; 120-min post-pneumoperitoneum and Trendelenburg position (T4): MD - 5.63, 95% CI - 7.35 to - 3.91, P < 0.01; Cydn, T2: MD 3.15, 1.53 to 4.77, P = 0.0001; T3: MD 2.78, 95% CI 1.43 to 4.14, P < 0.01] and PCV-VG (Ppeak, T2: MD - 3.99, 95% CI - 7.2 to - 0.78, P = 0.01; T3: MD - 3.46, 95% CI - 6.5 to - 0.42, P = 0.03; Cydn, T3: MD 4.44, 95% CI 2.23 to 6.66, P < 0.01; T4: MD 3.61, 95% CI 1.31 to 5.91, P = 0.002) significantly reduced Ppeak and improved Cydn compared with VCV after pneumoperitoneum and Trendelenburg position. PaO<sub>2</sub>, pH, and PaO<sub>2</sub>/FiO<sub>2</sub> did not differ between PCV and VCV or between PCV-VG and VCV during intraoperative surgery.</p><p><strong>Conclusions: </strong>Our meta-analysis suggests that in laparoscopic surgery in the Trendelenburg position, PCV or PCV-VG can provide a lower Ppeak and higher Cdyn throughout surgery but cannot offer better oxygenation than VCV. PCV or PCV-VG might be optimal for laparoscopic surgery in the Trendelenburg position.</p>","PeriodicalId":19764,"journal":{"name":"Perioperative Medicine","volume":"14 1","pages":"56"},"PeriodicalIF":2.1000,"publicationDate":"2025-05-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12070765/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Perioperative Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13741-025-00540-w","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Volume-controlled ventilation (VCV) and pressure-controlled ventilation (PCV) are commonly used in laparoscopic surgery in the Trendelenburg position, and pressure-controlled ventilation volume guaranteed (PCV-VG) has been increasingly used recently. However, there is still no consensus on the optimal ventilation mode. Therefore, a systematic review and meta-analysis were conducted to compare the effects of different ventilation modes for laparoscopic surgery in the Trendelenburg position.
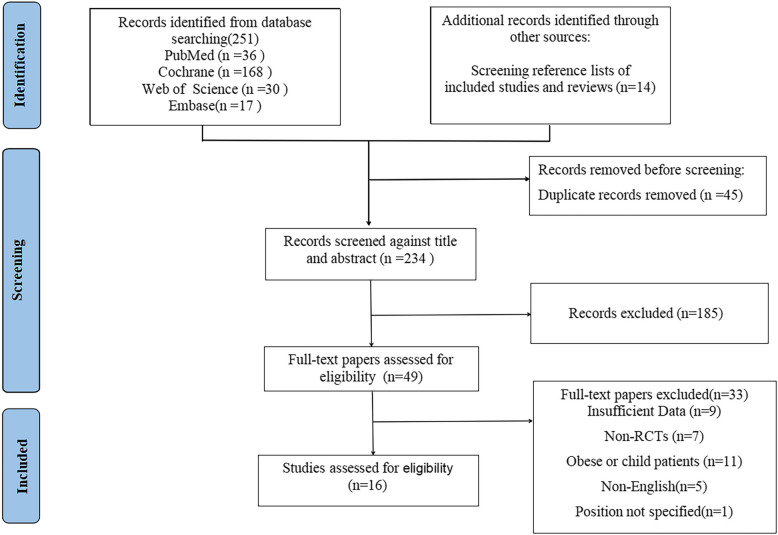
Methods: Multiple databases were searched for randomized controlled trials published before December 2024 to compare the effects of PCV, PCV-VG, and VCV in patients in the Trendelenburg position who underwent laparoscopic surgery. The primary outcomes included peak airway pressure (Ppeak), plateau airway pressure (Pplat), dynamic compliance (Cdyn), and blood gas analysis.
Results: Sixteen studies were included in this meta-analysis. PCV [Ppeak, 15‒40-min post-pneumoperitoneum and Trendelenburg position (T2): mean difference (MD) - 4.28, 95% confidence interval (CI) - 5.91 to - 2.64, P < 0.01; 60-min post-pneumoperitoneum and Trendelenburg position (T3): MD - 4.51, 95% CI - 5.41 to - 3.6, P < 0.01; 120-min post-pneumoperitoneum and Trendelenburg position (T4): MD - 5.63, 95% CI - 7.35 to - 3.91, P < 0.01; Cydn, T2: MD 3.15, 1.53 to 4.77, P = 0.0001; T3: MD 2.78, 95% CI 1.43 to 4.14, P < 0.01] and PCV-VG (Ppeak, T2: MD - 3.99, 95% CI - 7.2 to - 0.78, P = 0.01; T3: MD - 3.46, 95% CI - 6.5 to - 0.42, P = 0.03; Cydn, T3: MD 4.44, 95% CI 2.23 to 6.66, P < 0.01; T4: MD 3.61, 95% CI 1.31 to 5.91, P = 0.002) significantly reduced Ppeak and improved Cydn compared with VCV after pneumoperitoneum and Trendelenburg position. PaO2, pH, and PaO2/FiO2 did not differ between PCV and VCV or between PCV-VG and VCV during intraoperative surgery.
Conclusions: Our meta-analysis suggests that in laparoscopic surgery in the Trendelenburg position, PCV or PCV-VG can provide a lower Ppeak and higher Cdyn throughout surgery but cannot offer better oxygenation than VCV. PCV or PCV-VG might be optimal for laparoscopic surgery in the Trendelenburg position.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


