{"title":"A case of invasive pulmonary aspergillosis associated with clozapine-induced agranulocytosis.","authors":"Akiyoshi Yokode, Masaki Fujiwara, Toshiki Terao, Shinji Sakamoto, Yuto Yamada, Ryota Sato, Momoko Mishima, Yuji Yada, Ken-Ichi Matsuoka, Manabu Takaki","doi":"10.1002/pcn5.70077","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Clozapine-induced agranulocytosis (CLIA) is a rare but serious complication. Fever associated with CLIA is typically treated with broad-spectrum antimicrobials, but empiric antifungal therapy is rarely used. While bacterial and viral infections have been reported in CLIA cases, no cases of fungal infections complicated by CLIA have been documented. We report the first case of CLIA complicated by invasive pulmonary aspergillosis (IPA) in a patient with schizophrenia. The diagnosis of IPA was made using serum β-D-glucan, <i>Aspergillus</i> galactomannan antigen tests, and chest computed tomography (CT).</p><p><strong>Case presentation: </strong>We present a case of a 51-year-old man with schizophrenia who developed CLIA complicated by IPA. The patient, diagnosed with treatment-resistant schizophrenia, was started on clozapine, but 9 months later he presented with fever, cough, leukopenia, and neutropenia. Clozapine was discontinued, and empirical treatments with cefepime and filgrastim were initiated. Serum β-D-glucan and <i>Aspergillus</i> galactomannan antigen tests were positive, and chest CT showed well-circumscribed nodules, leading to a probable diagnosis of IPA. Antifungal therapy was switched from micafungin to voriconazole according to guidelines. His neutropenia and fever improved, and he was re-transferred to a psychiatric hospital.</p><p><strong>Conclusion: </strong>CLIA can be complicated by fungal infections. When patients with CLIA present with fever, fungal infections, including IPA, should be considered in the differential diagnosis. Serological tests, including β-D-glucan and <i>Aspergillus</i> galactomannan, are useful for the diagnosis of IPA as well as the appropriate use of antifungal agents in patients with CLIA.</p>","PeriodicalId":74405,"journal":{"name":"PCN reports : psychiatry and clinical neurosciences","volume":"4 1","pages":"e70077"},"PeriodicalIF":0.9000,"publicationDate":"2025-03-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12053896/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PCN reports : psychiatry and clinical neurosciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/pcn5.70077","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Clozapine-induced agranulocytosis (CLIA) is a rare but serious complication. Fever associated with CLIA is typically treated with broad-spectrum antimicrobials, but empiric antifungal therapy is rarely used. While bacterial and viral infections have been reported in CLIA cases, no cases of fungal infections complicated by CLIA have been documented. We report the first case of CLIA complicated by invasive pulmonary aspergillosis (IPA) in a patient with schizophrenia. The diagnosis of IPA was made using serum β-D-glucan, Aspergillus galactomannan antigen tests, and chest computed tomography (CT).
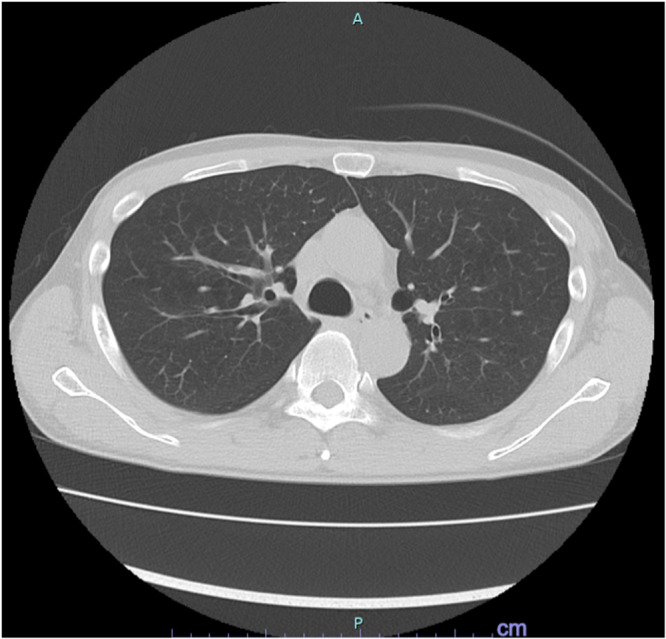
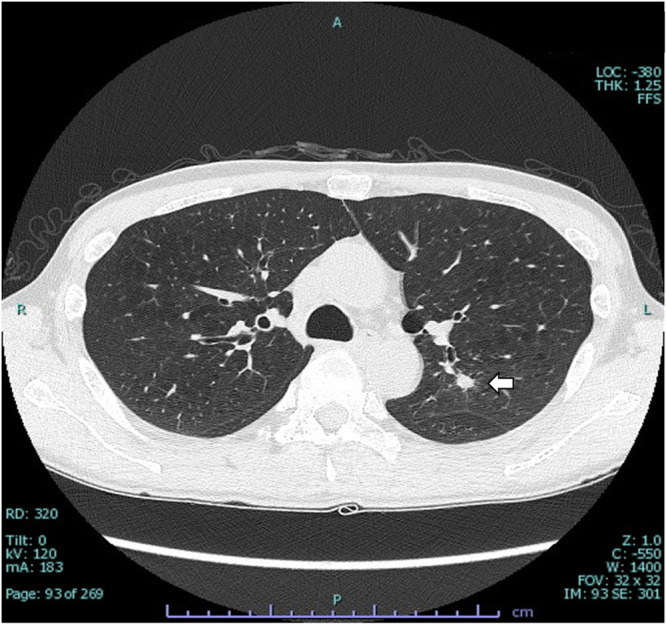
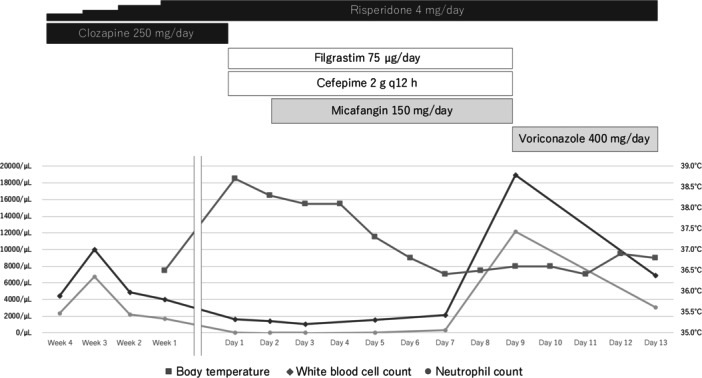
Case presentation: We present a case of a 51-year-old man with schizophrenia who developed CLIA complicated by IPA. The patient, diagnosed with treatment-resistant schizophrenia, was started on clozapine, but 9 months later he presented with fever, cough, leukopenia, and neutropenia. Clozapine was discontinued, and empirical treatments with cefepime and filgrastim were initiated. Serum β-D-glucan and Aspergillus galactomannan antigen tests were positive, and chest CT showed well-circumscribed nodules, leading to a probable diagnosis of IPA. Antifungal therapy was switched from micafungin to voriconazole according to guidelines. His neutropenia and fever improved, and he was re-transferred to a psychiatric hospital.
Conclusion: CLIA can be complicated by fungal infections. When patients with CLIA present with fever, fungal infections, including IPA, should be considered in the differential diagnosis. Serological tests, including β-D-glucan and Aspergillus galactomannan, are useful for the diagnosis of IPA as well as the appropriate use of antifungal agents in patients with CLIA.
背景:氯氮平所致粒细胞缺乏症(CLIA)是一种罕见但严重的并发症。与CLIA相关的发热通常用广谱抗菌剂治疗,但很少使用经验性抗真菌治疗。虽然在CLIA病例中有细菌和病毒感染的报道,但没有记录真菌感染并发CLIA的病例。我们报告了首例CLIA合并侵袭性肺曲霉病(IPA)的精神分裂症患者。采用血清β- d -葡聚糖、半乳甘露聚糖曲霉抗原检测及胸部CT诊断IPA。病例介绍:我们报告了一例51岁的精神分裂症患者,他发展为CLIA并IPA。该患者被诊断为难治性精神分裂症,开始服用氯氮平,但9个月后出现发烧、咳嗽、白细胞减少和中性粒细胞减少。停用氯氮平,开始使用头孢吡肟和非格拉西汀进行经经验治疗。血清β- d -葡聚糖和半乳甘露聚糖曲霉抗原检测阳性,胸部CT显示界限清晰的结节,可能诊断为IPA。根据指南将抗真菌治疗从米卡芬金转为伏立康唑。他的中性粒细胞减少症和发烧有所改善,他被重新转移到精神病院。结论:CLIA可并发真菌感染。当CLIA患者出现发热时,应考虑真菌感染,包括IPA,作为鉴别诊断。血清学测试,包括β- d -葡聚糖和半乳甘露聚糖曲霉,对IPA的诊断以及对CLIA患者适当使用抗真菌药物是有用的。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


