{"title":"Paraneoplastic Tumefactive Demyelination With Underlying Anaplastic Thyroid Cancer: A Case Report and Review of the Literature.","authors":"Chaloulos-Iakovidis Panagiotis, Arsany Hakim, Stork Lidia, Stadelmann-Nessler Christine, Kollár Attila, Chan Andrew, De Beukelaer Sophie, Salmen Anke, Hoepner Robert, Helly Hammer","doi":"10.1177/11795735251340051","DOIUrl":null,"url":null,"abstract":"<p><p>We present a case of paraneoplastic tumefactive demyelination in a 55-year-old female with an underlying anaplastic thyroid carcinoma (ATC), alongside a review of the literature on all cases of tumefactive demyelination associated with non-CNS neoplasia. In the presented case the patient developed a right-sided subacute sensorimotor hemiparesis. The initial cerebral MRI revealed a bilateral frontoparietal tumefactive mass lesion with marked gadolinium uptake and mass effect. Cerebrospinal fluid revealed CSF-specific oligoclonal bands type III, with negative cell count, protein and pathogen testing. Brain biopsy indicated demyelination and T-cell infiltrates and foamy macrophages. A body CT revealed an anaplastic thyroid carcinoma. Despite steroids, plasma exchange, rituximab, and cancer treatment, the patient died due to clinical fluctuation and cancer progression. In addition to our case 9 cases of tumefactive demyelinating have been reported in patients with newly diagnosed extracranial neoplasia, most commonly seminoma germ cell tumour (7/10). 8/10 (80%) of patients were male, with mean age at diagnosis was 52.9 years 95% C.I. [43.8, 62.0]. 5/10 patients presented with sensorimotor hemiparesis and/or confusion/neurocognitive deficits. 4/10 with visual deficits and 2/10 with aphasia. In all cases neoplasia was diagnosed simultaneously or after neurological manifestations. All cases presented initially as solitary lesions. A malignancy specific-treatment as well as steroid treatment in different regiments were applied. In addition in 2/10 plasmapheresis was implemented and 1/10 patients received intravenous immunoglobulins. In the majority of cases including the presented case partial neurological improvement was documented whereas malignancy usually progressed. To our knowledge, this is the first report of paraneoplastic tumefactive demyelination associated with an ATC highlighting the importance of a thorough workup in these patients. This is the first reported case of paraneoplastic tumefactive demyelination associated with ATC, underscoring the necessity of a comprehensive diagnostic approach in similar patients.</p>","PeriodicalId":15218,"journal":{"name":"Journal of Central Nervous System Disease","volume":"17 ","pages":"11795735251340051"},"PeriodicalIF":2.8000,"publicationDate":"2025-05-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12062606/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Central Nervous System Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795735251340051","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
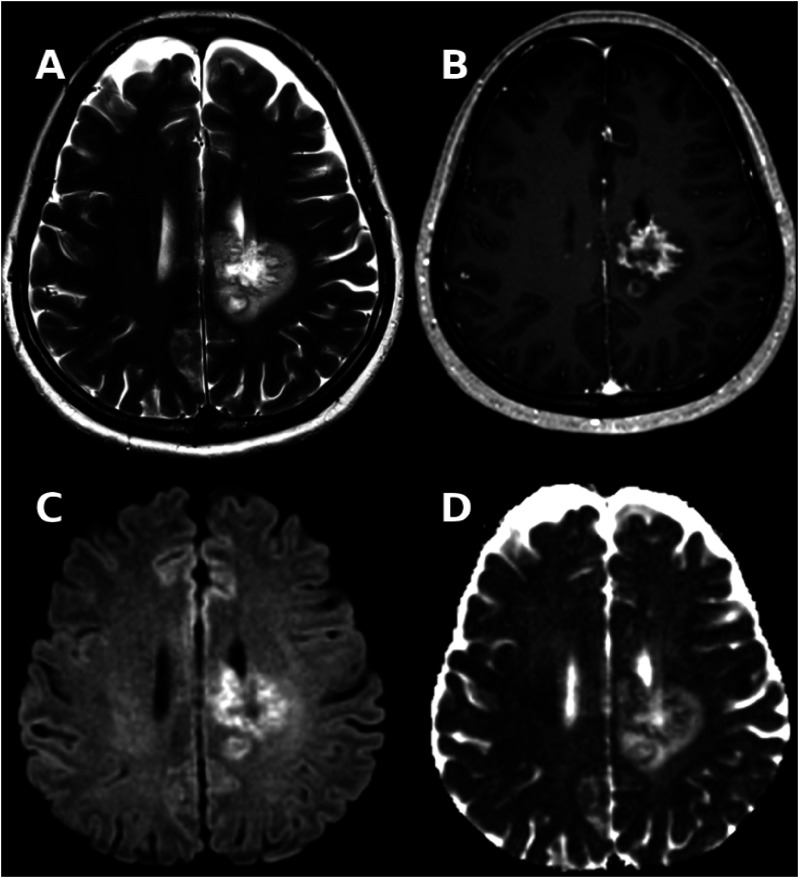
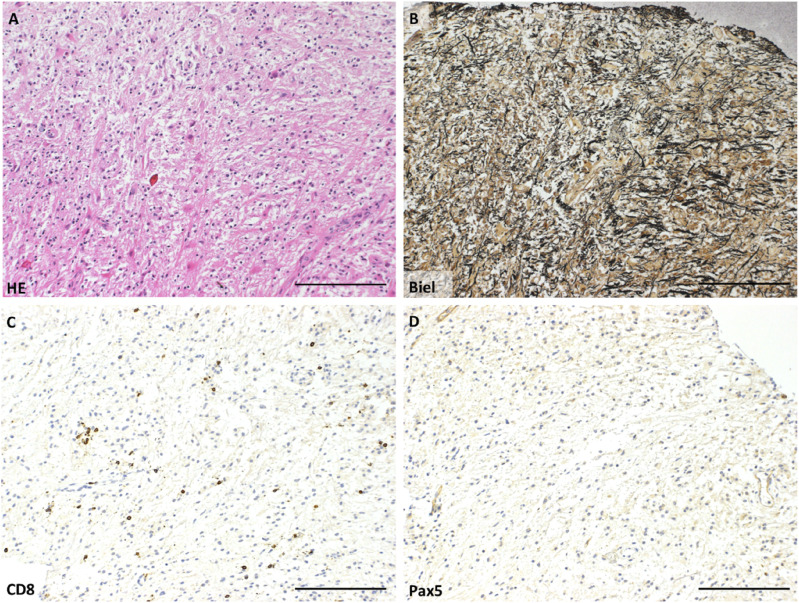
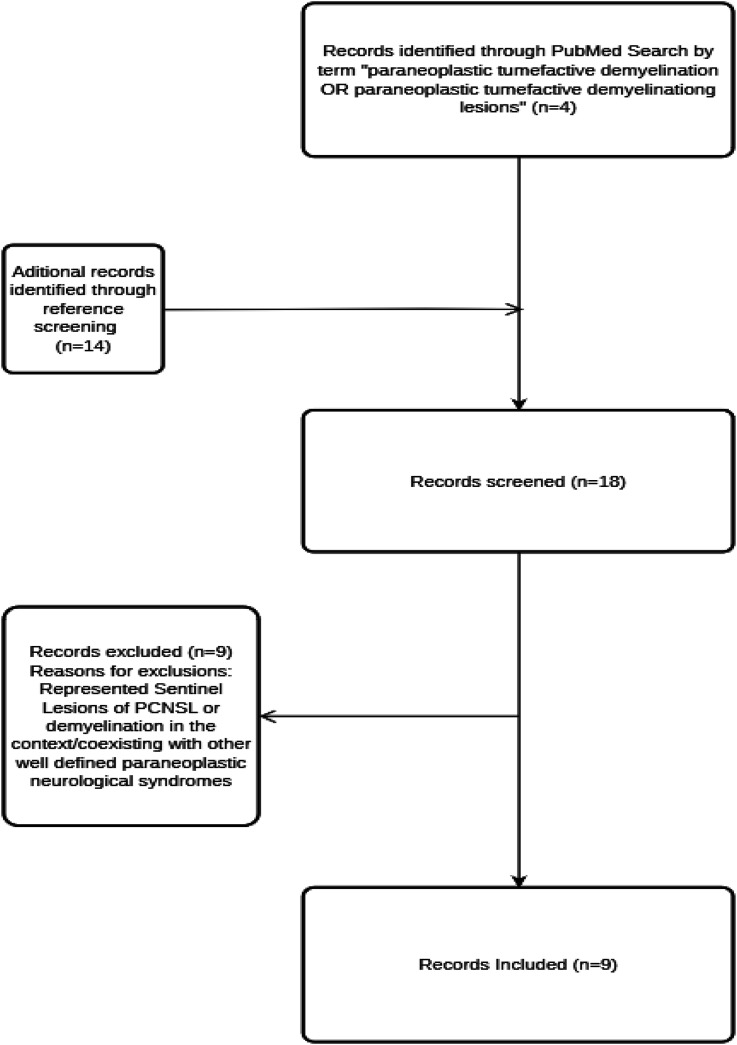
We present a case of paraneoplastic tumefactive demyelination in a 55-year-old female with an underlying anaplastic thyroid carcinoma (ATC), alongside a review of the literature on all cases of tumefactive demyelination associated with non-CNS neoplasia. In the presented case the patient developed a right-sided subacute sensorimotor hemiparesis. The initial cerebral MRI revealed a bilateral frontoparietal tumefactive mass lesion with marked gadolinium uptake and mass effect. Cerebrospinal fluid revealed CSF-specific oligoclonal bands type III, with negative cell count, protein and pathogen testing. Brain biopsy indicated demyelination and T-cell infiltrates and foamy macrophages. A body CT revealed an anaplastic thyroid carcinoma. Despite steroids, plasma exchange, rituximab, and cancer treatment, the patient died due to clinical fluctuation and cancer progression. In addition to our case 9 cases of tumefactive demyelinating have been reported in patients with newly diagnosed extracranial neoplasia, most commonly seminoma germ cell tumour (7/10). 8/10 (80%) of patients were male, with mean age at diagnosis was 52.9 years 95% C.I. [43.8, 62.0]. 5/10 patients presented with sensorimotor hemiparesis and/or confusion/neurocognitive deficits. 4/10 with visual deficits and 2/10 with aphasia. In all cases neoplasia was diagnosed simultaneously or after neurological manifestations. All cases presented initially as solitary lesions. A malignancy specific-treatment as well as steroid treatment in different regiments were applied. In addition in 2/10 plasmapheresis was implemented and 1/10 patients received intravenous immunoglobulins. In the majority of cases including the presented case partial neurological improvement was documented whereas malignancy usually progressed. To our knowledge, this is the first report of paraneoplastic tumefactive demyelination associated with an ATC highlighting the importance of a thorough workup in these patients. This is the first reported case of paraneoplastic tumefactive demyelination associated with ATC, underscoring the necessity of a comprehensive diagnostic approach in similar patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


