No additive effect of transcranial direct current stimulation on balance exercises for brain activity and clinical outcomes in patients with chronic ankle instability: a randomised controlled trial.
{"title":"No additive effect of transcranial direct current stimulation on balance exercises for brain activity and clinical outcomes in patients with chronic ankle instability: a randomised controlled trial.","authors":"Zivar Beyraghi, Roya Khanmohammadi","doi":"10.1136/bmjsem-2024-002401","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>This study explored whether adding transcranial direct current stimulation (tDCS) to balance exercises enhances preparatory brain activity and clinical outcomes in individuals with chronic ankle instability.</p><p><strong>Methods: </strong>30 participants were randomised into two groups: balance exercises with real tDCS and balance exercises with sham tDCS. Neurophysiological measures, including late contingent negative variation (CNV) amplitude, peak amplitude and peak time, served as primary outcomes, while biomechanical (anticipatory postural adjustment duration) and clinical (dynamic balance and perceived ankle instability) outcomes were secondary. Both groups completed 12 sessions, each lasting 60 min.</p><p><strong>Results: </strong>The results revealed no significant group-by-time interaction for late CNV amplitude, CNV peak amplitude, perceived ankle instability scores or dynamic balance, indicating no added benefit of real tDCS over sham. However, both groups demonstrated significant post-treatment improvements in late CNV amplitude (C3, Cz, C4: p≤0.017, η<sup>2</sup>=0.177-0.276) and CNV peak amplitude at the C3 electrode (p=0.026, η<sup>2</sup>=0.158), reflecting enhanced preparatory brain activity. Similarly, dynamic balance improved significantly in the anterior, posterior-medial and posterior-lateral directions (p≤0.010, η<sup>2</sup>=0.204-0.350) and perceived ankle instability scores increased notably, indicating reduced instability (p<0.001, η<sup>2</sup>=0.391), regardless of the tDCS condition. Furthermore, significant correlations (r=0.381-0.553) were observed between treatment-induced changes in neurophysiological variables and biomechanical and clinical outcomes.</p><p><strong>Conclusions: </strong>Although tDCS did not show a distinct advantage, the improvements in neurophysiological and clinical outcomes suggest that balance exercises effectively target central mechanisms. Additionally, relationships were found between enhancements in neurophysiological outcomes and other measures, emphasising the pivotal role of central mechanisms in driving these positive effects.</p><p><strong>Trial registration number: </strong>IRCT20210604051488N1.</p>","PeriodicalId":47417,"journal":{"name":"BMJ Open Sport & Exercise Medicine","volume":"11 2","pages":"e002401"},"PeriodicalIF":3.2000,"publicationDate":"2025-04-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11987147/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Sport & Exercise Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjsem-2024-002401","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"SPORT SCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: This study explored whether adding transcranial direct current stimulation (tDCS) to balance exercises enhances preparatory brain activity and clinical outcomes in individuals with chronic ankle instability.
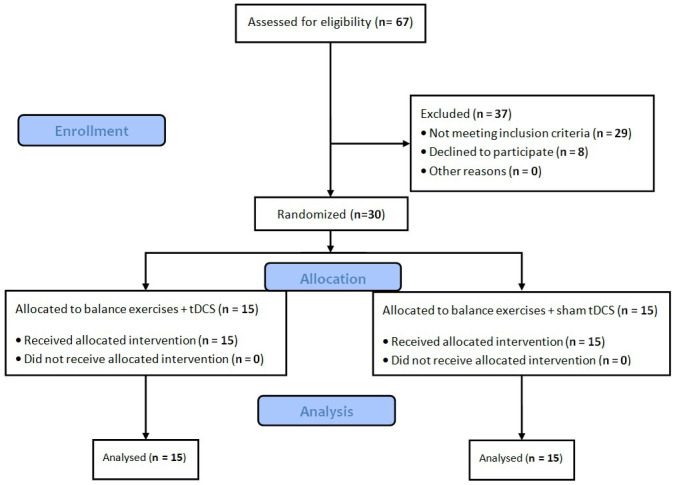
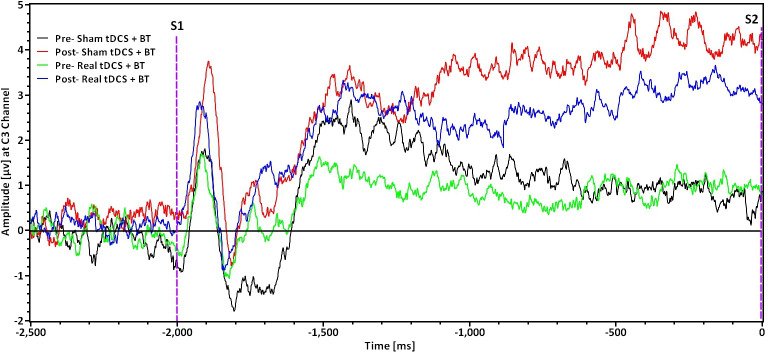
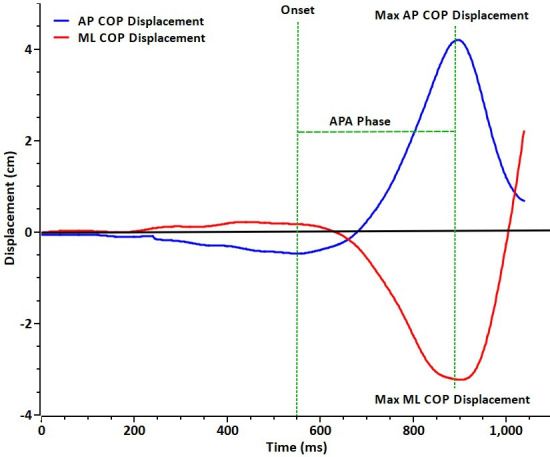
Methods: 30 participants were randomised into two groups: balance exercises with real tDCS and balance exercises with sham tDCS. Neurophysiological measures, including late contingent negative variation (CNV) amplitude, peak amplitude and peak time, served as primary outcomes, while biomechanical (anticipatory postural adjustment duration) and clinical (dynamic balance and perceived ankle instability) outcomes were secondary. Both groups completed 12 sessions, each lasting 60 min.
Results: The results revealed no significant group-by-time interaction for late CNV amplitude, CNV peak amplitude, perceived ankle instability scores or dynamic balance, indicating no added benefit of real tDCS over sham. However, both groups demonstrated significant post-treatment improvements in late CNV amplitude (C3, Cz, C4: p≤0.017, η2=0.177-0.276) and CNV peak amplitude at the C3 electrode (p=0.026, η2=0.158), reflecting enhanced preparatory brain activity. Similarly, dynamic balance improved significantly in the anterior, posterior-medial and posterior-lateral directions (p≤0.010, η2=0.204-0.350) and perceived ankle instability scores increased notably, indicating reduced instability (p<0.001, η2=0.391), regardless of the tDCS condition. Furthermore, significant correlations (r=0.381-0.553) were observed between treatment-induced changes in neurophysiological variables and biomechanical and clinical outcomes.
Conclusions: Although tDCS did not show a distinct advantage, the improvements in neurophysiological and clinical outcomes suggest that balance exercises effectively target central mechanisms. Additionally, relationships were found between enhancements in neurophysiological outcomes and other measures, emphasising the pivotal role of central mechanisms in driving these positive effects.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


