Yağmur Seda Yeşiltaş, Zackery Oakey, Jennifer Brainard, Gabrielle Yeaney, Arun D Singh
{"title":"Necrotic iris melanocytoma with secondary glaucoma.","authors":"Yağmur Seda Yeşiltaş, Zackery Oakey, Jennifer Brainard, Gabrielle Yeaney, Arun D Singh","doi":"10.4103/tjo.TJO-D-24-00126","DOIUrl":null,"url":null,"abstract":"<p><p>A 54-year-old female was referred because of a pigmented iris lesion with uncontrolled glaucoma in the left eye. The intraocular pressure (IOP) was 54 mm Hg despite anti-glaucoma medications. Her visual acuity (VA) was 20/100. A slit-lamp examination showed corneal edema and a darkly pigmented small iridociliary lesion (Ultrasound biomicroscopy: 5 mm × 3 mm × 2 mm) with diffuse pigment shedding onto the anterior iris surface and diffuse circumferential pigmentation of the trabecular meshwork with wide-open angle (gonioscopy). Diagnostic fine needle aspiration biopsy of the main tumor and anterior chamber lavage were performed. Cytology revealed polygonal cells with dense intracytoplasmic pigment obscuring nuclear details diagnostic of a melanocytoma. During follow-up, as the tumor continued to cause new pigment shedding with high IOP, therefore, excision of the primary tumor via iridocyclectomy was performed. At postoperative 1 month, the IOP was 13 mm Hg with maximal medical therapy for glaucoma requiring glaucoma shunt surgery. At 6 months, the IOP remained below 13 mm Hg and the VA was 20/50 without recurrence of pigment shedding. Necrotic iris melanocytoma, though rare, can lead to pigment dispersion glaucoma. Surgical excision of the primary tumor, coupled with glaucoma surgery, proved effective in controlling intraocular pressure and preserving vision in this case.</p>","PeriodicalId":44978,"journal":{"name":"Taiwan Journal of Ophthalmology","volume":"15 1","pages":"135-137"},"PeriodicalIF":1.2000,"publicationDate":"2025-01-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11981570/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Taiwan Journal of Ophthalmology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/tjo.TJO-D-24-00126","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"OPHTHALMOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
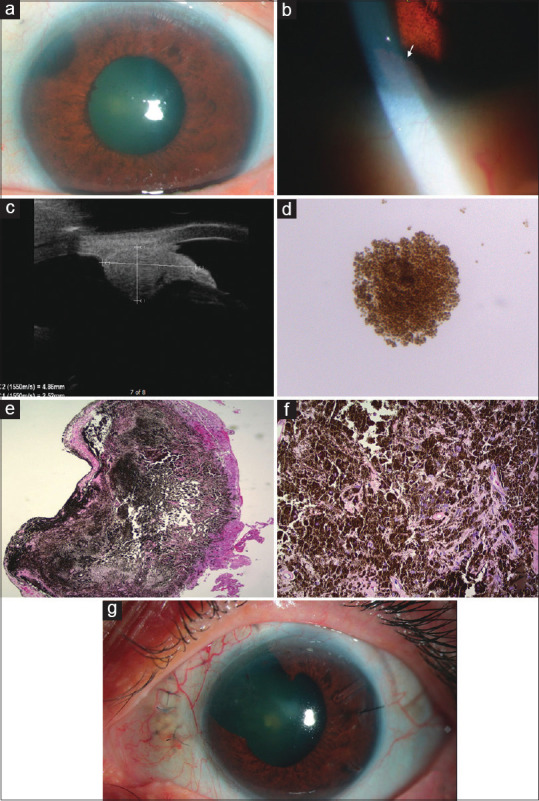
A 54-year-old female was referred because of a pigmented iris lesion with uncontrolled glaucoma in the left eye. The intraocular pressure (IOP) was 54 mm Hg despite anti-glaucoma medications. Her visual acuity (VA) was 20/100. A slit-lamp examination showed corneal edema and a darkly pigmented small iridociliary lesion (Ultrasound biomicroscopy: 5 mm × 3 mm × 2 mm) with diffuse pigment shedding onto the anterior iris surface and diffuse circumferential pigmentation of the trabecular meshwork with wide-open angle (gonioscopy). Diagnostic fine needle aspiration biopsy of the main tumor and anterior chamber lavage were performed. Cytology revealed polygonal cells with dense intracytoplasmic pigment obscuring nuclear details diagnostic of a melanocytoma. During follow-up, as the tumor continued to cause new pigment shedding with high IOP, therefore, excision of the primary tumor via iridocyclectomy was performed. At postoperative 1 month, the IOP was 13 mm Hg with maximal medical therapy for glaucoma requiring glaucoma shunt surgery. At 6 months, the IOP remained below 13 mm Hg and the VA was 20/50 without recurrence of pigment shedding. Necrotic iris melanocytoma, though rare, can lead to pigment dispersion glaucoma. Surgical excision of the primary tumor, coupled with glaucoma surgery, proved effective in controlling intraocular pressure and preserving vision in this case.
一位54岁女性因左眼色素性虹膜病变伴不受控制的青光眼而被转诊。尽管服用了抗青光眼药物,但眼压(IOP)仍为54 mm Hg。视力(VA)为20/100。裂隙灯检查显示角膜水肿,虹膜小病变颜色深(超声生物显微镜:5 mm × 3 mm × 2 mm),虹膜前表面弥漫性色素脱落,大开角(角镜)小梁网弥漫性周向色素沉着。主要肿瘤行诊断性细针穿刺活检及前房灌洗。细胞学检查显示多角形细胞内有致密的胞浆内色素,模糊了细胞核细节,诊断为黑色素细胞瘤。在随访中,由于肿瘤继续引起新的色素脱落,且IOP较高,因此,通过虹膜环切除术切除原发肿瘤。术后1个月,IOP为13 mm Hg,青光眼的最大药物治疗需要青光眼分流手术。6个月时,IOP保持在13 mm Hg以下,VA为20/50,无色素脱落复发。坏死性虹膜黑色素细胞瘤虽然罕见,但可导致色素性青光眼。手术切除原发肿瘤,再加上青光眼手术,证明在控制眼压和保留视力方面是有效的。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


