Anton Pozniak, Chloe Orkin, Yazdan Yazdanpanah, Axel Baumgarten, Karam Mounzer, Michelle L D'Antoni, Hailin Huang, Hui Liu, Kristen Andreatta, Laurie A VanderVeen, Christian Callebaut, Jason T Hindman, José R Arribas
{"title":"Efficacy of Bictegravir/Emtricitabine/Tenofovir Alafenamide (B/F/TAF) After A Viremic Event: A Pooled Analysis of Studies in People with HIV.","authors":"Anton Pozniak, Chloe Orkin, Yazdan Yazdanpanah, Axel Baumgarten, Karam Mounzer, Michelle L D'Antoni, Hailin Huang, Hui Liu, Kristen Andreatta, Laurie A VanderVeen, Christian Callebaut, Jason T Hindman, José R Arribas","doi":"10.1007/s40121-025-01153-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Transient viremia can occur in people with human immunodeficiency virus (HIV), often referred to as people with HIV (PWH), and is sometimes related to poor adherence to antiretroviral therapy (ART). Guidelines recommend achieving virologic resuppression with existing ART regimens while addressing the reasons for the lack of virologic control. However, there are limited clinical trial data on the effectiveness of the strategy of continuing the same ART regimen in treatment-experienced PWH following a period of viremia. This was a post hoc pooled analysis of eight clinical studies in PWH receiving bictegravir/emtricitabine/tenofovir alafenamide (B/F/TAF).</p><p><strong>Methods: </strong>Viremic events occurring in participants receiving B/F/TAF were defined as ≥ 1 viral load (VL) measurement of ≥ 50 copies/mL after virologic suppression (VL < 50 copies/mL). Outcomes after viremic events were categorized as: virologic resuppression (≥ 1 subsequent VL < 50 copies/mL); continued viremia (all subsequent VLs ≥ 50 copies/mL); or not evaluable (no subsequent VL assessment). Adherence was calculated by pill count from returned pill bottles.</p><p><strong>Results: </strong>The analysis included 2801 participants. A total of 411 viremic events were experienced by 290 participants, 50% of whom were treatment naïve at B/F/TAF initiation, and the other 50% were virologically suppressed. A total of 91 participants experienced ≥ 1 viremic event of ≥ 1000 copies/mL. The proportion of viremic events followed by resuppression on B/F/TAF was 90.3%, rising to 96.6% when nonevaluable data were excluded. The median (quartile [Q]1, Q3) time from a viremic event to documented resuppression was 22 (18, 36) days. Among 13 participants with continued viremia, 11 (84.6%) prematurely discontinued B/F/TAF. No treatment-emergent resistance was observed in participants with continued viremia. A significantly higher proportion of participants with a viremic event had < 85% adherence compared with those without (10.0% and 4.2%, respectively; p = 0.0003).</p><p><strong>Conclusions: </strong>Most participants receiving B/F/TAF experienced no viremic events. The vast majority of viremic events resolved with B/F/TAF continuation, without the need for treatment change.</p>","PeriodicalId":13592,"journal":{"name":"Infectious Diseases and Therapy","volume":" ","pages":"1201-1217"},"PeriodicalIF":5.3000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12151942/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious Diseases and Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40121-025-01153-y","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/15 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
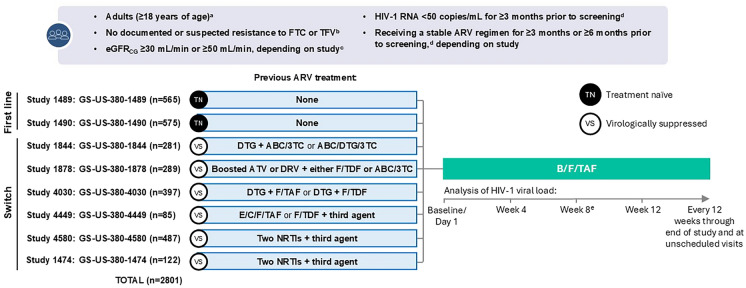
Introduction: Transient viremia can occur in people with human immunodeficiency virus (HIV), often referred to as people with HIV (PWH), and is sometimes related to poor adherence to antiretroviral therapy (ART). Guidelines recommend achieving virologic resuppression with existing ART regimens while addressing the reasons for the lack of virologic control. However, there are limited clinical trial data on the effectiveness of the strategy of continuing the same ART regimen in treatment-experienced PWH following a period of viremia. This was a post hoc pooled analysis of eight clinical studies in PWH receiving bictegravir/emtricitabine/tenofovir alafenamide (B/F/TAF).
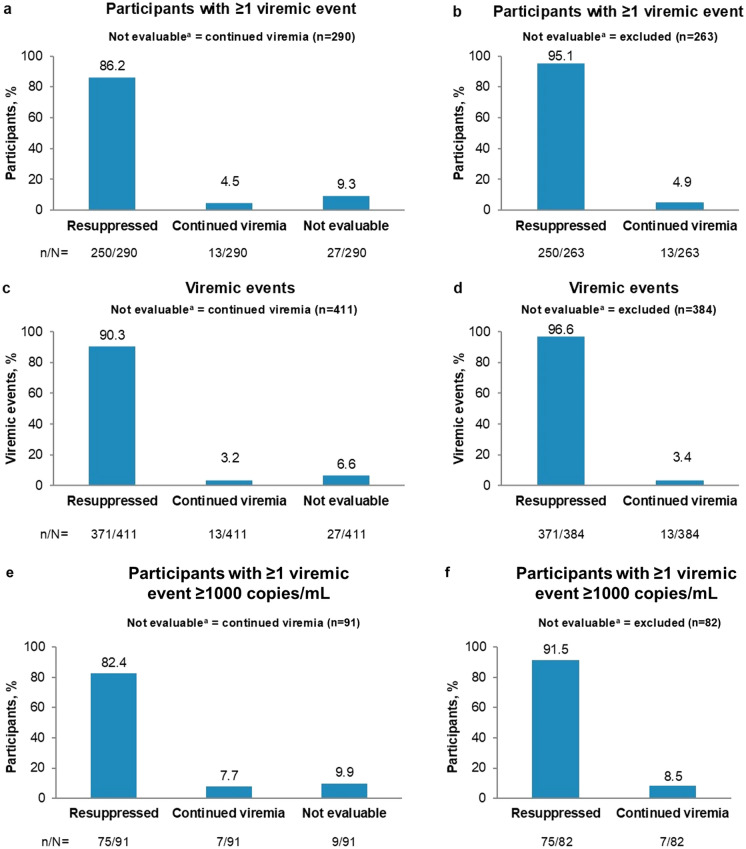
Methods: Viremic events occurring in participants receiving B/F/TAF were defined as ≥ 1 viral load (VL) measurement of ≥ 50 copies/mL after virologic suppression (VL < 50 copies/mL). Outcomes after viremic events were categorized as: virologic resuppression (≥ 1 subsequent VL < 50 copies/mL); continued viremia (all subsequent VLs ≥ 50 copies/mL); or not evaluable (no subsequent VL assessment). Adherence was calculated by pill count from returned pill bottles.
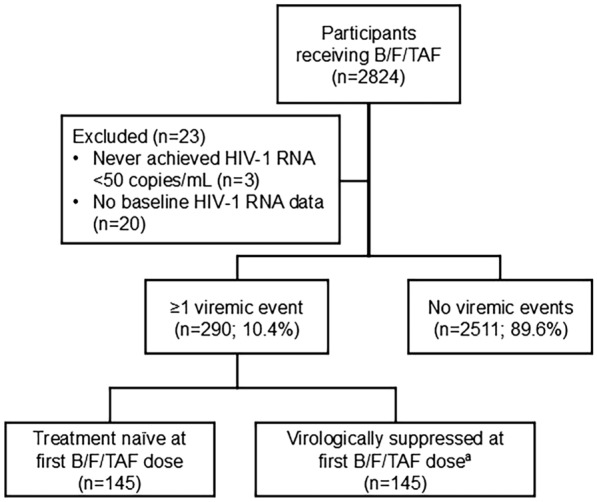
Results: The analysis included 2801 participants. A total of 411 viremic events were experienced by 290 participants, 50% of whom were treatment naïve at B/F/TAF initiation, and the other 50% were virologically suppressed. A total of 91 participants experienced ≥ 1 viremic event of ≥ 1000 copies/mL. The proportion of viremic events followed by resuppression on B/F/TAF was 90.3%, rising to 96.6% when nonevaluable data were excluded. The median (quartile [Q]1, Q3) time from a viremic event to documented resuppression was 22 (18, 36) days. Among 13 participants with continued viremia, 11 (84.6%) prematurely discontinued B/F/TAF. No treatment-emergent resistance was observed in participants with continued viremia. A significantly higher proportion of participants with a viremic event had < 85% adherence compared with those without (10.0% and 4.2%, respectively; p = 0.0003).
Conclusions: Most participants receiving B/F/TAF experienced no viremic events. The vast majority of viremic events resolved with B/F/TAF continuation, without the need for treatment change.
期刊介绍:
Infectious Diseases and Therapy is an international, open access, peer-reviewed, rapid publication journal dedicated to the publication of high-quality clinical (all phases), observational, real-world, and health outcomes research around the discovery, development, and use of infectious disease therapies and interventions, including vaccines and devices. Studies relating to diagnostic products and diagnosis, pharmacoeconomics, public health, epidemiology, quality of life, and patient care, management, and education are also encouraged.
Areas of focus include, but are not limited to, bacterial and fungal infections, viral infections (including HIV/AIDS and hepatitis), parasitological diseases, tuberculosis and other mycobacterial diseases, vaccinations and other interventions, and drug-resistance, chronic infections, epidemiology and tropical, emergent, pediatric, dermal and sexually-transmitted diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


