The impact of medication reconciliation on discrepancies and all-cause readmission among hospitalised patients with chronic kidney disease: a quasi-experimental study.
Shoroq M Altawalbeh, Nahlah M Sallam, Osama Y Alshogran, Minas Al-Khatib, Mohammad S Bani Amer, Linda Tahaineh, Abla Albsoul-Younes
{"title":"The impact of medication reconciliation on discrepancies and all-cause readmission among hospitalised patients with chronic kidney disease: a quasi-experimental study.","authors":"Shoroq M Altawalbeh, Nahlah M Sallam, Osama Y Alshogran, Minas Al-Khatib, Mohammad S Bani Amer, Linda Tahaineh, Abla Albsoul-Younes","doi":"10.1080/20523211.2025.2488173","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Chronic kidney disease (CKD) with its associated comorbidities and pill burden can expose patients to a heightened risk of drug-related problems, including medication discrepancies. This study aimed to evaluate the impact of medication reconciliation supplemented with medication review on the number of medication discrepancies at discharge and all-cause readmission among CKD patients.</p><p><strong>Methods: </strong>This was a quasi-experimental trial among adult CKD patients admitted into two major referral hospitals in northern Jordan. Patients in the intervention group received medication reconciliation supplemented with medication review by a clinical pharmacist, while those in the control group received the usual care. The recognised discrepancies were evaluated at admission and at discharge in both groups. Participants were followed for 90-day readmission.</p><p><strong>Results: </strong>Among patients in the intervention group, the average number of discrepancies was 2.5 ± 2.2 per CKD patient. Compared to the control group, the reduction in discrepancy numbers between admission and discharge was higher in the intervention group by 1.66 discrepancies. The likelihood of 90-day readmission was significantly lower in the intervention group (OR = 0.41; <i>P</i> = 0.002).</p><p><strong>Conclusion: </strong>Supplemented medication reconciliation among CKD patients reveals a favourable impact on medication discrepancies and readmission rates. Optimising medication management during transitions of care can improve overall health outcomes.</p>","PeriodicalId":16740,"journal":{"name":"Journal of Pharmaceutical Policy and Practice","volume":"18 1","pages":"2488173"},"PeriodicalIF":2.5000,"publicationDate":"2025-04-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11998305/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Pharmaceutical Policy and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/20523211.2025.2488173","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
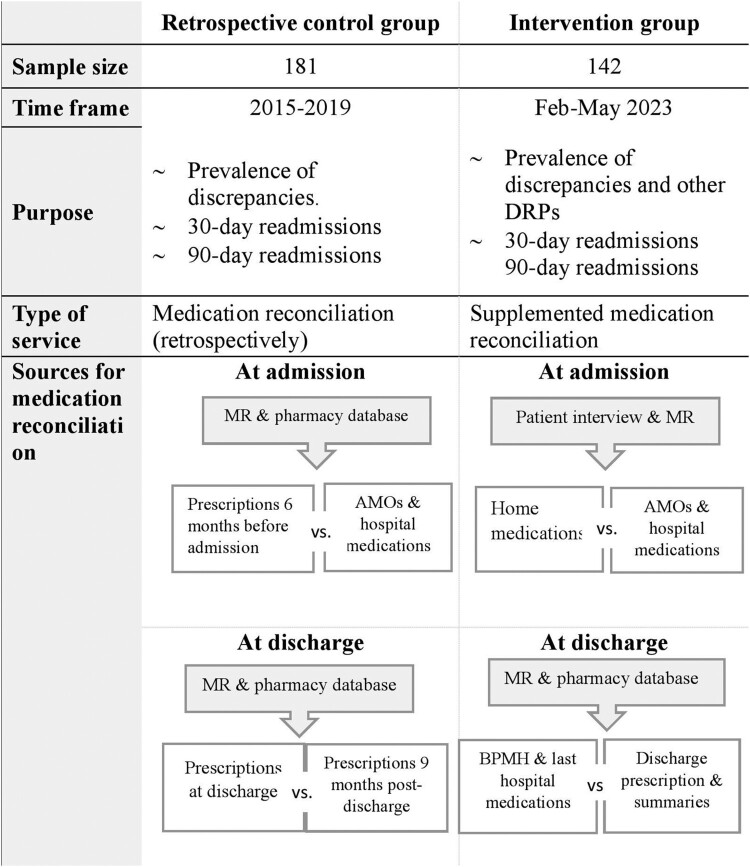
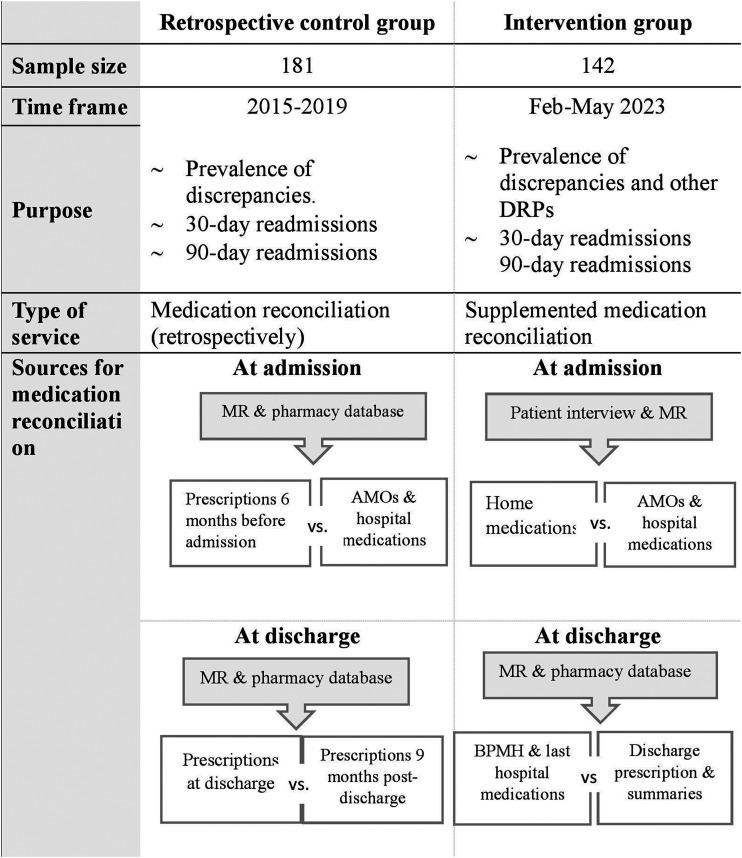
Background: Chronic kidney disease (CKD) with its associated comorbidities and pill burden can expose patients to a heightened risk of drug-related problems, including medication discrepancies. This study aimed to evaluate the impact of medication reconciliation supplemented with medication review on the number of medication discrepancies at discharge and all-cause readmission among CKD patients.
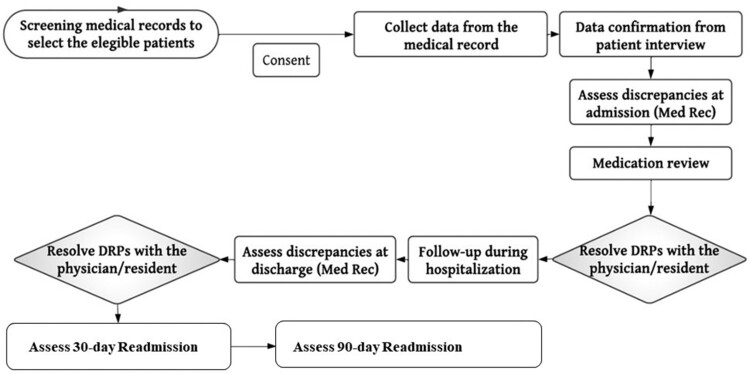
Methods: This was a quasi-experimental trial among adult CKD patients admitted into two major referral hospitals in northern Jordan. Patients in the intervention group received medication reconciliation supplemented with medication review by a clinical pharmacist, while those in the control group received the usual care. The recognised discrepancies were evaluated at admission and at discharge in both groups. Participants were followed for 90-day readmission.
Results: Among patients in the intervention group, the average number of discrepancies was 2.5 ± 2.2 per CKD patient. Compared to the control group, the reduction in discrepancy numbers between admission and discharge was higher in the intervention group by 1.66 discrepancies. The likelihood of 90-day readmission was significantly lower in the intervention group (OR = 0.41; P = 0.002).
Conclusion: Supplemented medication reconciliation among CKD patients reveals a favourable impact on medication discrepancies and readmission rates. Optimising medication management during transitions of care can improve overall health outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


