Yash Akkara, Joshua J Hon, Mahathir Ahmed, Basel Musmar, Joanna Roy, Stavropoula Tjoumakaris, Michael Reid Gooch, Robert H Rosenwasser, Pascal Jabbour
{"title":"Cost-Effectiveness of Carotid Endarterectomy vs. Carotid Stenting: a Systematic Review and Meta-Analysis.","authors":"Yash Akkara, Joshua J Hon, Mahathir Ahmed, Basel Musmar, Joanna Roy, Stavropoula Tjoumakaris, Michael Reid Gooch, Robert H Rosenwasser, Pascal Jabbour","doi":"10.1007/s12975-025-01347-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Carotid artery stenting (CAS) and carotid endarterectomy (CEA) are gold-standard treatments of carotid artery stenosis. This study aims to identify the cost-effectiveness of CEA vs CAS.</p><p><strong>Methods: </strong>Studies were screened through PubMed, MEDLINE, and Embase using PRISMA guidelines, and required ≥ 20 participants who were ≥ 16 years, alongside costs at 1-year postoperatively. The Shapiro-Wilk test, independent sample t-tests, ANOVA, and Spearman's R were used, with costs adjusted to 2024. A random-effects model was used to compare cost-effectiveness. Bias assessment was according to the Cochrane Risk of Bias 2.0 tool and the Newcastle-Ottawa Scale.</p><p><strong>Results: </strong>7 studies were included, with a sample of 6493 participants (3418 M, 3075 F). 2932 and 3511 participants underwent CEA and CAS respectively. CEA reported a significantly longer mean length of procedure (191.92 vs. 77.5 min, p < 0.0001) and length of stay (3.13 vs. 2.60 days, p < 0.0001) vs. CAS. The mean adjusted cost of CEA and CAS were $18156.60 (6466) and $17711.01 (5511) respectively. Studies reported lower risks of stroke (2.12% vs. 3.65%, p < 0.001), higher risks of myocardial infarctions (1.70% vs. 1.42%, p < 0.01), and higher risks of other complications for CEA vs. CAS respectively. The expected 1-year cost of CEA was marginally lower than CAS ($21264.03 vs. $21433.14, p < 0.05). The cost-effectiveness of CEA was marginally better than CAS (ratio = 1.019, 95% CI [1.017, 1.020)].</p><p><strong>Conclusions: </strong>CEA provides marginally improved cost-effectiveness over CAS, providing long-term cost benefits to centers with large surgical volumes. However, shorter procedural times and inpatient stays with CAS may improve overall productivity. Cost should hence not be a deciding factor when choosing between CEA and CAS.</p>","PeriodicalId":23237,"journal":{"name":"Translational Stroke Research","volume":" ","pages":"1874-1883"},"PeriodicalIF":4.3000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12391230/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational Stroke Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12975-025-01347-z","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/11 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Carotid artery stenting (CAS) and carotid endarterectomy (CEA) are gold-standard treatments of carotid artery stenosis. This study aims to identify the cost-effectiveness of CEA vs CAS.
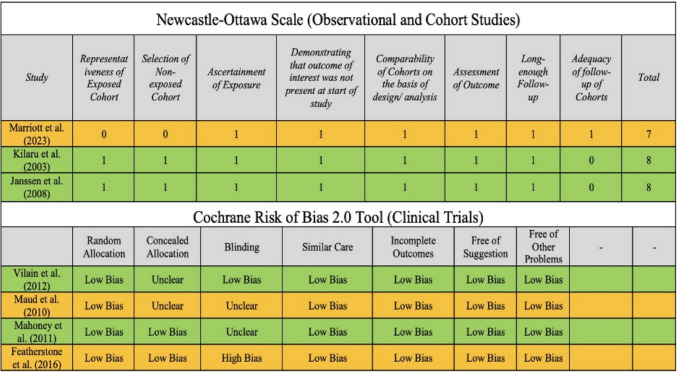
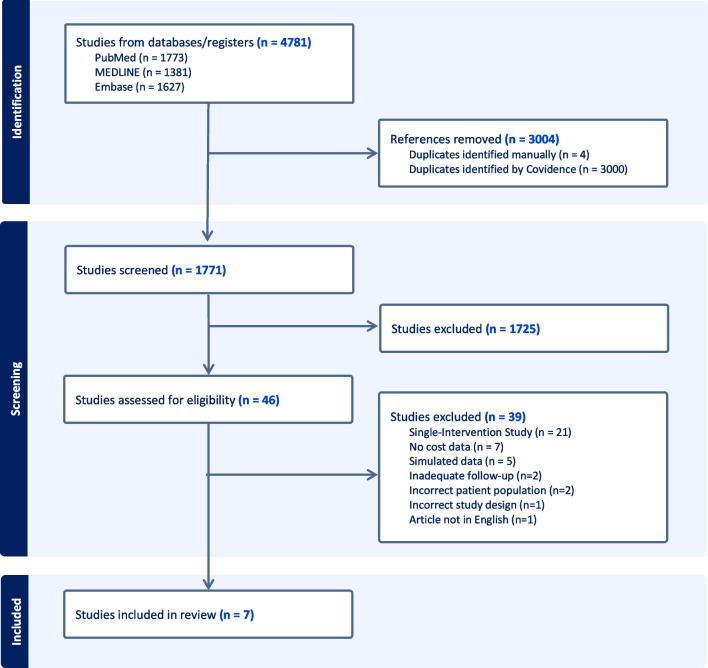
Methods: Studies were screened through PubMed, MEDLINE, and Embase using PRISMA guidelines, and required ≥ 20 participants who were ≥ 16 years, alongside costs at 1-year postoperatively. The Shapiro-Wilk test, independent sample t-tests, ANOVA, and Spearman's R were used, with costs adjusted to 2024. A random-effects model was used to compare cost-effectiveness. Bias assessment was according to the Cochrane Risk of Bias 2.0 tool and the Newcastle-Ottawa Scale.
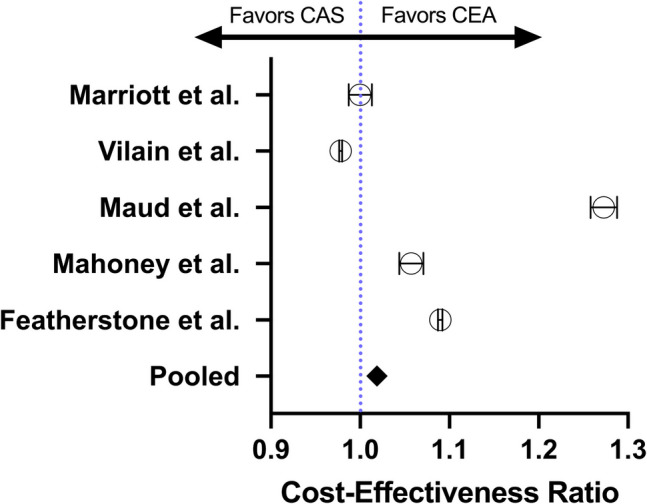
Results: 7 studies were included, with a sample of 6493 participants (3418 M, 3075 F). 2932 and 3511 participants underwent CEA and CAS respectively. CEA reported a significantly longer mean length of procedure (191.92 vs. 77.5 min, p < 0.0001) and length of stay (3.13 vs. 2.60 days, p < 0.0001) vs. CAS. The mean adjusted cost of CEA and CAS were $18156.60 (6466) and $17711.01 (5511) respectively. Studies reported lower risks of stroke (2.12% vs. 3.65%, p < 0.001), higher risks of myocardial infarctions (1.70% vs. 1.42%, p < 0.01), and higher risks of other complications for CEA vs. CAS respectively. The expected 1-year cost of CEA was marginally lower than CAS ($21264.03 vs. $21433.14, p < 0.05). The cost-effectiveness of CEA was marginally better than CAS (ratio = 1.019, 95% CI [1.017, 1.020)].
Conclusions: CEA provides marginally improved cost-effectiveness over CAS, providing long-term cost benefits to centers with large surgical volumes. However, shorter procedural times and inpatient stays with CAS may improve overall productivity. Cost should hence not be a deciding factor when choosing between CEA and CAS.
期刊介绍:
Translational Stroke Research covers basic, translational, and clinical studies. The Journal emphasizes novel approaches to help both to understand clinical phenomenon through basic science tools, and to translate basic science discoveries into the development of new strategies for the prevention, assessment, treatment, and enhancement of central nervous system repair after stroke and other forms of neurotrauma.
Translational Stroke Research focuses on translational research and is relevant to both basic scientists and physicians, including but not restricted to neuroscientists, vascular biologists, neurologists, neuroimagers, and neurosurgeons.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


