M Abdelmonem, M Elsayed, D Awadallah, O Don, R H Bennett, O G Mackay, S Pookayil, C Archer, M Mahgoub, M J Bennett
{"title":"The impact of frailty on functional recovery after cardiac surgery-a case control study.","authors":"M Abdelmonem, M Elsayed, D Awadallah, O Don, R H Bennett, O G Mackay, S Pookayil, C Archer, M Mahgoub, M J Bennett","doi":"10.1186/s13741-025-00526-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Good functional recovery after cardiac surgery can be reported as 'days alive and out of hospital' in the first 30 days after a procedure (DAOH<sub>30</sub>) and 'days at home' in the first year (DAH<sub>365</sub>), which integrate several clinically important outcomes, including death, hospital length of stay, quality of recovery and hospital readmission. They depend on the preservation or early recovery of physiological and functional capacity, both of which may be lost in patients living with frailty.</p><p><strong>Case presentation: </strong>We measured frailty with a multidimensional approach, incorporating 30 variables spanning comorbidity, sensory, cognitive, psychosocial, disability and pharmaceutical domains, which together make up the Patient Frailty Index (pFI). We further explored the impact of socioeconomic factors on functional recovery using the Welsh Index of Multiple Deprivation (WIMD). The outcome measures included duration of level 3 and level 2 care, duration of hospital stay, readmission and both short- and longer-term mortality. A total of 669 patients were included in the final analysis. A total of 224 (33.5%) of the patients were 'frail'. They were more likely to have chronic obstructive pulmonary disease, heart failure and diabetes and to be in the lowest decile for deprivation. Frailty was not associated with either sex or advanced age. Patients deemed to be 'frail' had a longer stay in intensive care, required level 3 cardiovascular and respiratory support for longer and stayed longer in the hospital. They spent fewer days at home in the first 30 days, largely due to days requiring advanced cardiovascular support, and fewer days at home in the first year, with most days lost to patients who died in the first year following their surgery. A moderation analysis examined whether the WIMD modified the effect of frailty on recovery after cardiac surgery. The interaction term, after confirming there were no collinearity concerns, was not significant, either for DAOH<sub>30</sub> or DAH<sub>365</sub>, indicating no evidence of moderation.</p><p><strong>Conclusions: </strong>Short- and medium-term measures of good functional recovery were lower in 'frail' patients, and longer-term survival was also significantly reduced. An accumulation of deficits assessment of frailty, incorporating multiple domains, builds a more accurate picture of increasing vulnerability and can be acquired from patients' electronic health records. In a surgical population that is increasingly comorbid, these findings should inform decisions on preoperative priority setting, prehabilitation, postoperative resources and discharge planning.</p>","PeriodicalId":19764,"journal":{"name":"Perioperative Medicine","volume":"14 1","pages":"46"},"PeriodicalIF":2.1000,"publicationDate":"2025-04-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12016124/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Perioperative Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13741-025-00526-8","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Good functional recovery after cardiac surgery can be reported as 'days alive and out of hospital' in the first 30 days after a procedure (DAOH30) and 'days at home' in the first year (DAH365), which integrate several clinically important outcomes, including death, hospital length of stay, quality of recovery and hospital readmission. They depend on the preservation or early recovery of physiological and functional capacity, both of which may be lost in patients living with frailty.
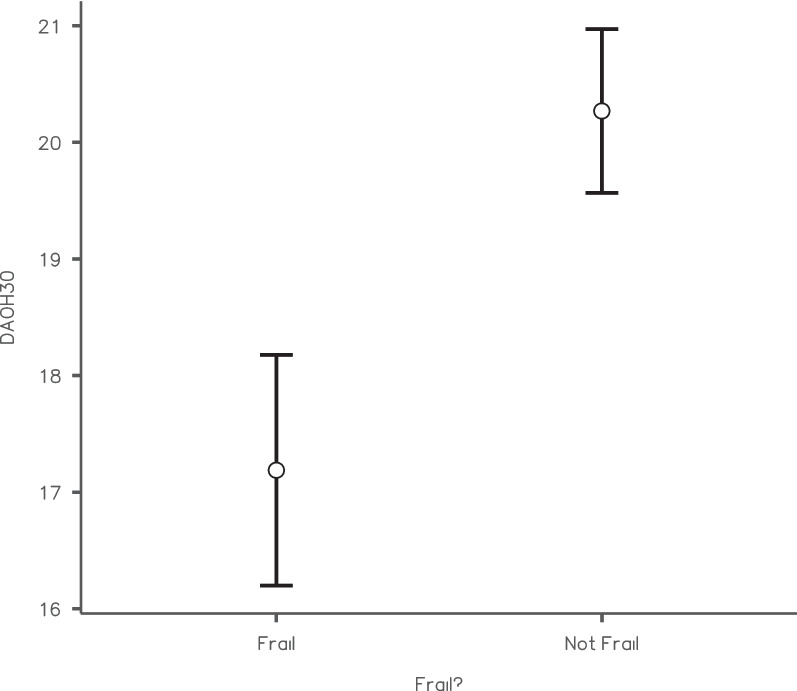
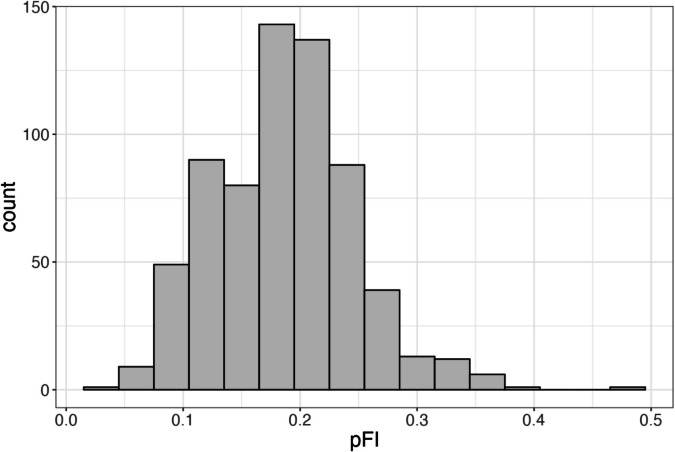
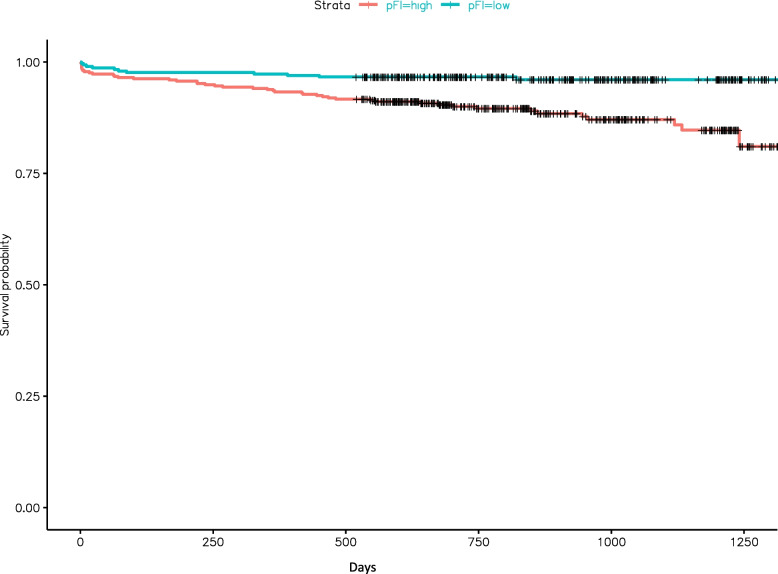
Case presentation: We measured frailty with a multidimensional approach, incorporating 30 variables spanning comorbidity, sensory, cognitive, psychosocial, disability and pharmaceutical domains, which together make up the Patient Frailty Index (pFI). We further explored the impact of socioeconomic factors on functional recovery using the Welsh Index of Multiple Deprivation (WIMD). The outcome measures included duration of level 3 and level 2 care, duration of hospital stay, readmission and both short- and longer-term mortality. A total of 669 patients were included in the final analysis. A total of 224 (33.5%) of the patients were 'frail'. They were more likely to have chronic obstructive pulmonary disease, heart failure and diabetes and to be in the lowest decile for deprivation. Frailty was not associated with either sex or advanced age. Patients deemed to be 'frail' had a longer stay in intensive care, required level 3 cardiovascular and respiratory support for longer and stayed longer in the hospital. They spent fewer days at home in the first 30 days, largely due to days requiring advanced cardiovascular support, and fewer days at home in the first year, with most days lost to patients who died in the first year following their surgery. A moderation analysis examined whether the WIMD modified the effect of frailty on recovery after cardiac surgery. The interaction term, after confirming there were no collinearity concerns, was not significant, either for DAOH30 or DAH365, indicating no evidence of moderation.
Conclusions: Short- and medium-term measures of good functional recovery were lower in 'frail' patients, and longer-term survival was also significantly reduced. An accumulation of deficits assessment of frailty, incorporating multiple domains, builds a more accurate picture of increasing vulnerability and can be acquired from patients' electronic health records. In a surgical population that is increasingly comorbid, these findings should inform decisions on preoperative priority setting, prehabilitation, postoperative resources and discharge planning.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


