Effects of mandibular setback surgery using the surgery-first approach versus conventional orthognathic approach on upper airway change and sleep quality.
{"title":"Effects of mandibular setback surgery using the surgery-first approach versus conventional orthognathic approach on upper airway change and sleep quality.","authors":"Wichuda Kongsong, Sunisa Rochanavibhata, Chidsanu Changsiripun, Phonkit Sinpitaksakul, Naricha Chirakalwasan","doi":"10.1186/s13005-025-00517-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To compare the effects of mandibular setback surgery on the upper airway and sleep quality using two approaches: the surgery-first approach (SFA) and the conventional orthognathic approach (COA).</p><p><strong>Materials and methods: </strong>A prospective, comparative clinical study was conducted in 20 patients, with 10 in each group undergoing isolated mandibular setback surgery. Three-dimensional upper airway analysis using cone-beam computed tomography and sleep quality assessments through questionnaires and sleep studies were performed preoperatively (T0), within 1 month postoperatively (T1), and six months postoperatively (T2).</p><p><strong>Results: </strong>The SFA group demonstrated greater mandibular setback and rotational changes compared to the COA group. Both groups exhibited postoperative reductions in airway volume and minimum cross-sectional area, with no significant intergroup differences. Significant differences in the change in airway length in the upper airway segment (0.9 ± 1.0 mm for SFA vs. -1.2 ± 3.4 mm for COA, P = 0.002) and total airway length (3.3 ± 1.8 mm for SFA vs. -0.1 ± 2.3 mm for COA, P < 0.001) were observed at T2 compared to the preoperative period. Subjective and objective sleep parameters were comparable between the groups. Objective sleep quality initially worsened but improved over time.</p><p><strong>Conclusions: </strong>Isolated mandibular setback surgery, whether performed using SFA or COA, resulted in comparable changes in upper airway dimensions and sleep quality.</p><p><strong>Clinical relevance: </strong>The choice between SFA and COA for isolated mandibular setback surgery does not significantly influence surgical decision-making regarding upper airway changes and sleep quality.</p>","PeriodicalId":12994,"journal":{"name":"Head & Face Medicine","volume":"21 1","pages":"37"},"PeriodicalIF":2.4000,"publicationDate":"2025-05-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12065383/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Head & Face Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13005-025-00517-6","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"DENTISTRY, ORAL SURGERY & MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To compare the effects of mandibular setback surgery on the upper airway and sleep quality using two approaches: the surgery-first approach (SFA) and the conventional orthognathic approach (COA).
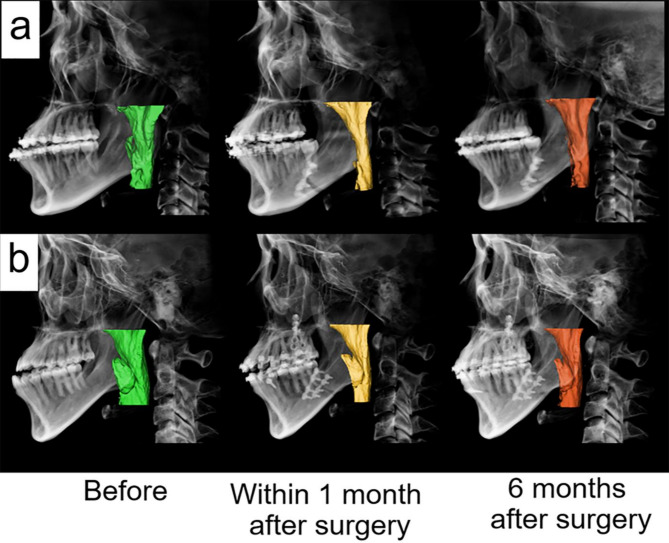
Materials and methods: A prospective, comparative clinical study was conducted in 20 patients, with 10 in each group undergoing isolated mandibular setback surgery. Three-dimensional upper airway analysis using cone-beam computed tomography and sleep quality assessments through questionnaires and sleep studies were performed preoperatively (T0), within 1 month postoperatively (T1), and six months postoperatively (T2).
Results: The SFA group demonstrated greater mandibular setback and rotational changes compared to the COA group. Both groups exhibited postoperative reductions in airway volume and minimum cross-sectional area, with no significant intergroup differences. Significant differences in the change in airway length in the upper airway segment (0.9 ± 1.0 mm for SFA vs. -1.2 ± 3.4 mm for COA, P = 0.002) and total airway length (3.3 ± 1.8 mm for SFA vs. -0.1 ± 2.3 mm for COA, P < 0.001) were observed at T2 compared to the preoperative period. Subjective and objective sleep parameters were comparable between the groups. Objective sleep quality initially worsened but improved over time.
Conclusions: Isolated mandibular setback surgery, whether performed using SFA or COA, resulted in comparable changes in upper airway dimensions and sleep quality.
Clinical relevance: The choice between SFA and COA for isolated mandibular setback surgery does not significantly influence surgical decision-making regarding upper airway changes and sleep quality.
期刊介绍:
Head & Face Medicine is a multidisciplinary open access journal that publishes basic and clinical research concerning all aspects of cranial, facial and oral conditions.
The journal covers all aspects of cranial, facial and oral diseases and their management. It has been designed as a multidisciplinary journal for clinicians and researchers involved in the diagnostic and therapeutic aspects of diseases which affect the human head and face. The journal is wide-ranging, covering the development, aetiology, epidemiology and therapy of head and face diseases to the basic science that underlies these diseases. Management of head and face diseases includes all aspects of surgical and non-surgical treatments including psychopharmacological therapies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


