{"title":"Rethinking antibiotic prophylaxis in orthopaedic oncology: insights from a cohort study of endoprosthetic infections.","authors":"Tariq Azamgarhi, Craig Gerrand, Simon Warren","doi":"10.5194/jbji-10-33-2025","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction</b>: Endoprosthetic replacement (EPR) is the preferred limb salvage method for musculoskeletal tumours involving bone; however, infection rates range from 8 % to 12 %. We investigated the impact of antibiotic prophylaxis at primary implantation on the development of prosthetic joint infection (PJI). <b>Methods</b>: We conducted a retrospective analysis of patients who underwent primary EPRs between 2010 and 2021. Prosthetic joint infections were identified and classified according to criteria from the European Bone and Joint Infection Society (EBJIS). The follow-up period extended until an infection was identified, subsequent surgery for non-infectious reasons occurred or the last known follow-up was conducted. For all primary procedures, we collected details of postoperative complications at the surgical site, including superficial wound infections, delayed wound healing and wound dehiscence. PJIs were divided into two groups. The first group included patients with an uncomplicated postoperative course, while the second comprised those with either postoperative wound problems or infections from an identifiable source. <b>Results</b>: Out of 1064 patients, 73 (6.9 %) developed PJI within a median follow-up of 25.6 months (IQR 8.8-52.7). A total of 26 % of PJIs were attributed to primary implantation, while 74 % of PJIs were due to secondary causes, with 47 % having wound complications and 27 % presenting acutely. The microbiological profiles between groups differed significantly, with infections from skin flora related to primary implantation and a high proportion of other bacteria (Gram-negatives and enterococci) linked to secondary infections. <b>Conclusions</b>: Skin flora are likely responsible for infections related to the primary procedure, and antibiotic prophylaxis should be optimised accordingly. Additional measures are needed to prevent secondary infections.</p>","PeriodicalId":15271,"journal":{"name":"Journal of Bone and Joint Infection","volume":"10 1","pages":"33-39"},"PeriodicalIF":2.8000,"publicationDate":"2025-02-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12050981/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Bone and Joint Infection","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5194/jbji-10-33-2025","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
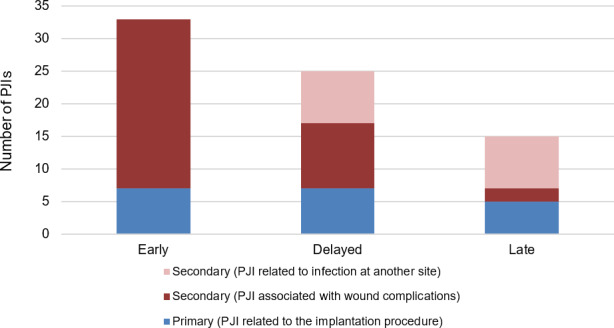
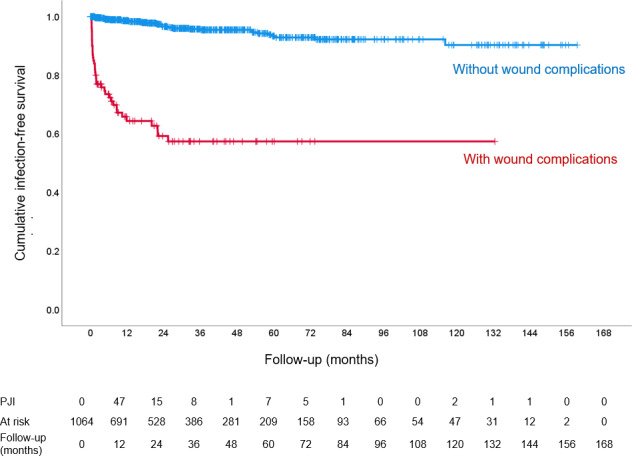
Introduction: Endoprosthetic replacement (EPR) is the preferred limb salvage method for musculoskeletal tumours involving bone; however, infection rates range from 8 % to 12 %. We investigated the impact of antibiotic prophylaxis at primary implantation on the development of prosthetic joint infection (PJI). Methods: We conducted a retrospective analysis of patients who underwent primary EPRs between 2010 and 2021. Prosthetic joint infections were identified and classified according to criteria from the European Bone and Joint Infection Society (EBJIS). The follow-up period extended until an infection was identified, subsequent surgery for non-infectious reasons occurred or the last known follow-up was conducted. For all primary procedures, we collected details of postoperative complications at the surgical site, including superficial wound infections, delayed wound healing and wound dehiscence. PJIs were divided into two groups. The first group included patients with an uncomplicated postoperative course, while the second comprised those with either postoperative wound problems or infections from an identifiable source. Results: Out of 1064 patients, 73 (6.9 %) developed PJI within a median follow-up of 25.6 months (IQR 8.8-52.7). A total of 26 % of PJIs were attributed to primary implantation, while 74 % of PJIs were due to secondary causes, with 47 % having wound complications and 27 % presenting acutely. The microbiological profiles between groups differed significantly, with infections from skin flora related to primary implantation and a high proportion of other bacteria (Gram-negatives and enterococci) linked to secondary infections. Conclusions: Skin flora are likely responsible for infections related to the primary procedure, and antibiotic prophylaxis should be optimised accordingly. Additional measures are needed to prevent secondary infections.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


