Effects of Blood Flow Restriction Training on Strength and Functionality in People With Knee Arthropathies: A Systematic Review and Dose-Response Meta-Analysis of Randomized Controlled Trials.
Daniel C Ogrezeanu, Luís Suso-Martí, Rubén López-Bueno, Pedro Gargallo, Rodrigo Núñez-Cortés, Carlos Cruz-Montecinos, Lars Louis Andersen, José Casaña, Nicholas Rolnick, Joaquín Calatayud
{"title":"Effects of Blood Flow Restriction Training on Strength and Functionality in People With Knee Arthropathies: A Systematic Review and Dose-Response Meta-Analysis of Randomized Controlled Trials.","authors":"Daniel C Ogrezeanu, Luís Suso-Martí, Rubén López-Bueno, Pedro Gargallo, Rodrigo Núñez-Cortés, Carlos Cruz-Montecinos, Lars Louis Andersen, José Casaña, Nicholas Rolnick, Joaquín Calatayud","doi":"10.1155/tsm2/3663009","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Previous meta-analyses show contrasting findings regarding the effects of blood flow restriction training (BFRT) in different knee conditions. Furthermore, no previous dose-response analysis has been conducted to determine the dose of BFRT required for maximal strength and functionality adaptations. <b>Objective:</b> To analyze the evidence on the effects of BFRT on strength and functionality in patients with knee osteoarthritis or rheumatoid arthritis through a systematic review with dose-response meta-analysis. <b>Methods:</b> Included studies met the following criteria: participants with knee osteoarthritis or rheumatoid arthritis; low-load resistance BFRT as intervention; control group with traditional moderate or high intensity resistance training (MIRT and HIRT); include muscle strength and functionality as primary and secondary outcome measures, respectively; and only randomized controlled trials. A random-effects and a dose-response model estimated strength and functionality using estimates of the total repetitions performed. <b>Results:</b> We included five studies with a sample of 205 participants. No statistically significant differences were found between BFRT and MIRT or HIRT for strength (SMD = -0.06; 95% CI = -0.78-0.67; and <i>p</i> > 0.05) and functionality (SMD = 0.07; 95% CI = -0.23-0.37; and <i>p</i> > 0.05). We found an inverted U-shaped association between the increase in total repetitions and strength gain and between the increase in total repetitions and functional improvement. <b>Conclusions:</b> People with knee osteoarthritis or rheumatoid arthritis can use low-load BFRT for strength and functionality as a similarly effective alternative to MIRT and HIRT. A total of 2000 repetitions per BFRT program are necessary to maximize strength gains in these patients, while functional improvement requires 1800 total repetitions.</p>","PeriodicalId":75247,"journal":{"name":"Translational sports medicine","volume":"2025 ","pages":"3663009"},"PeriodicalIF":1.9000,"publicationDate":"2025-04-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12006712/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational sports medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/tsm2/3663009","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SPORT SCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
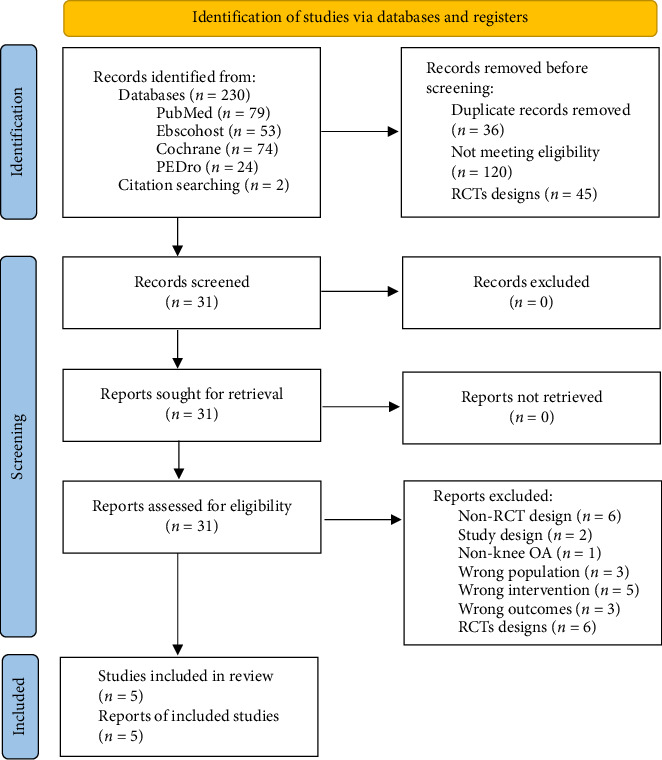
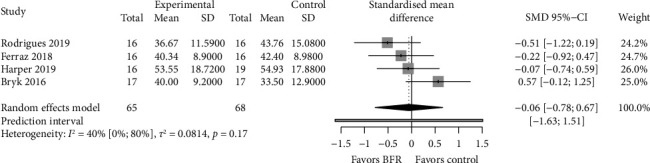
Background: Previous meta-analyses show contrasting findings regarding the effects of blood flow restriction training (BFRT) in different knee conditions. Furthermore, no previous dose-response analysis has been conducted to determine the dose of BFRT required for maximal strength and functionality adaptations. Objective: To analyze the evidence on the effects of BFRT on strength and functionality in patients with knee osteoarthritis or rheumatoid arthritis through a systematic review with dose-response meta-analysis. Methods: Included studies met the following criteria: participants with knee osteoarthritis or rheumatoid arthritis; low-load resistance BFRT as intervention; control group with traditional moderate or high intensity resistance training (MIRT and HIRT); include muscle strength and functionality as primary and secondary outcome measures, respectively; and only randomized controlled trials. A random-effects and a dose-response model estimated strength and functionality using estimates of the total repetitions performed. Results: We included five studies with a sample of 205 participants. No statistically significant differences were found between BFRT and MIRT or HIRT for strength (SMD = -0.06; 95% CI = -0.78-0.67; and p > 0.05) and functionality (SMD = 0.07; 95% CI = -0.23-0.37; and p > 0.05). We found an inverted U-shaped association between the increase in total repetitions and strength gain and between the increase in total repetitions and functional improvement. Conclusions: People with knee osteoarthritis or rheumatoid arthritis can use low-load BFRT for strength and functionality as a similarly effective alternative to MIRT and HIRT. A total of 2000 repetitions per BFRT program are necessary to maximize strength gains in these patients, while functional improvement requires 1800 total repetitions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


