Comparison of robotic, conventional, and endoscopic nipple-sparing mastectomy with immediate prosthetic breast reconstruction for breast cancer: A systematic review and meta-analysis.
Na An, Wenjuan Wang, Dandan Dai, Fei Yuan, Yufeng Zhang
{"title":"Comparison of robotic, conventional, and endoscopic nipple-sparing mastectomy with immediate prosthetic breast reconstruction for breast cancer: A systematic review and meta-analysis.","authors":"Na An, Wenjuan Wang, Dandan Dai, Fei Yuan, Yufeng Zhang","doi":"10.17305/bb.2025.11687","DOIUrl":null,"url":null,"abstract":"<p><p>In this network meta-analysis (NMA), we aimed to evaluate the relative efficacy of robotic nipple-sparing mastectomy (RNSM), conventional nipple-sparing mastectomy (CNSM), and endoscope-assisted nipple-sparing mastectomy (ENSM), each combined with immediate prosthetic breast reconstruction (IPBR), for the treatment of breast cancer. Relevant studies published up to June 15, 2024, were identified through searches of PubMed, Embase, the Cochrane Library, and Web of Science. Data extracted from these studies were analyzed using Stata 15.1 and the Gemtc 1.0.1 package in R 4.2.3. A Bayesian framework and a Markov Chain Monte Carlo model were employed to conduct the NMA. Additionally, a ranking chart was generated to compare the advantages and disadvantages of the surgical methods. Ten studies met the inclusion criteria and were included in the NMA. The results indicated that ENSM with immediate implant-based reconstruction was associated with a smaller incision compared to CNSM. RNSM combined with IPBR was linked to a lower incidence of total complications, Grade 3 complications, and nipple-areola complex necrosis than CNSM. Furthermore, RNSM with IPBR demonstrated a lower recurrence rate than CNSM. However, CNSM with IPBR showed better outcomes in terms of surgical time, hospital stay, and positive margin infiltration. In contrast, RNSM and ENSM, both combined with IPBR, outperformed CNSM in terms of incision length, complication rates, and recurrence outcomes.</p>","PeriodicalId":72398,"journal":{"name":"Biomolecules & biomedicine","volume":" ","pages":"1737-1750"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12447740/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Biomolecules & biomedicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17305/bb.2025.11687","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"0","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 0
Abstract
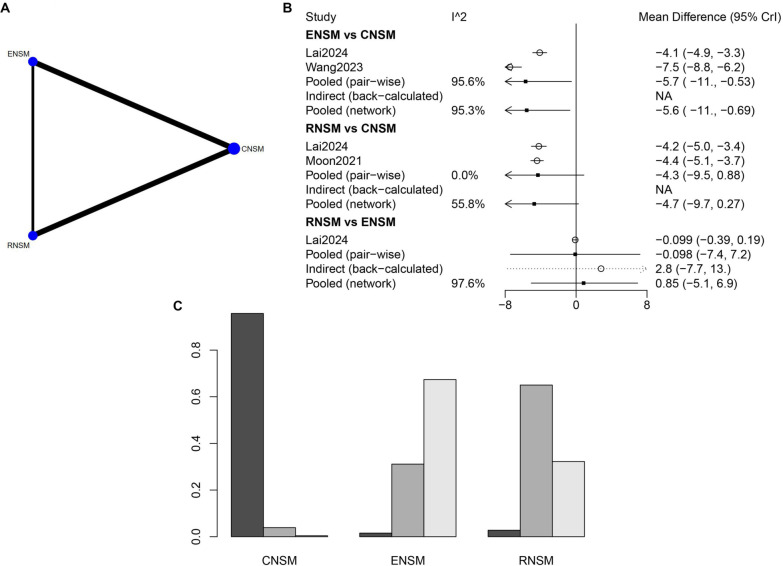
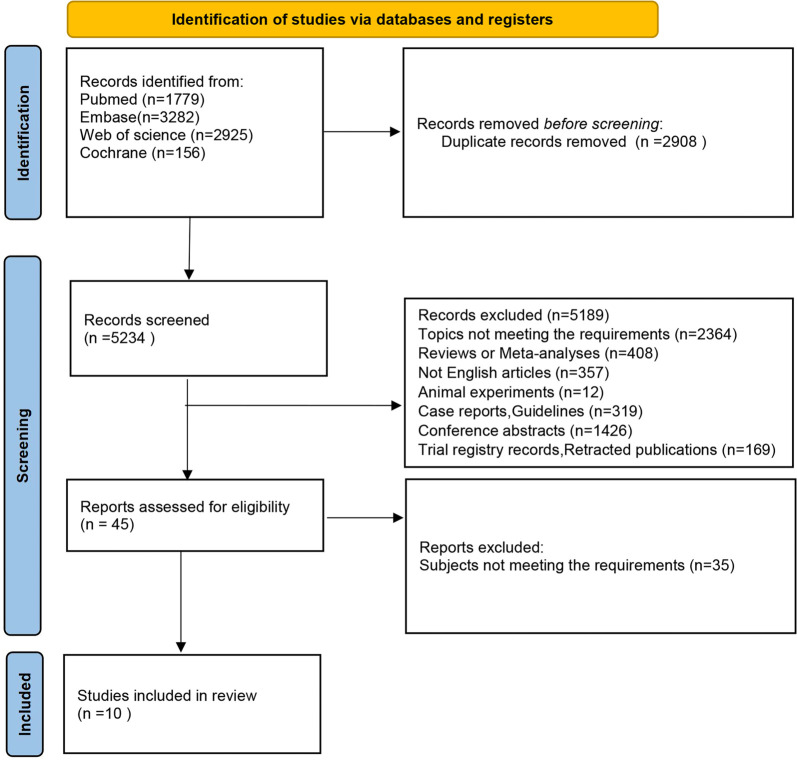
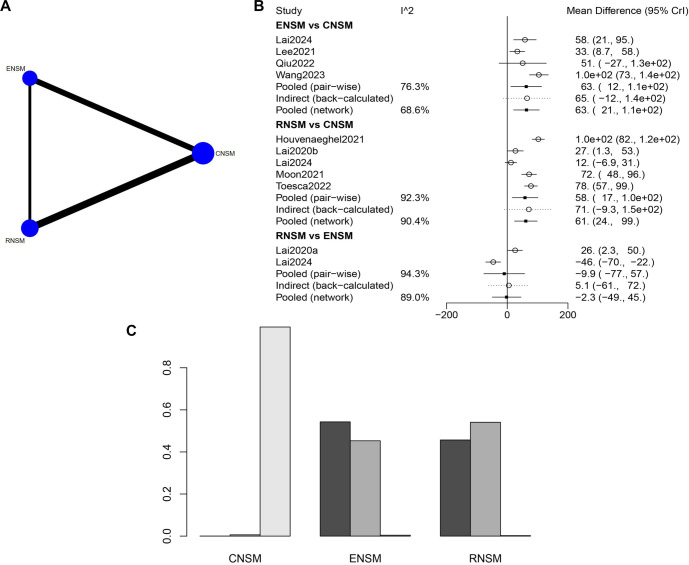
In this network meta-analysis (NMA), we aimed to evaluate the relative efficacy of robotic nipple-sparing mastectomy (RNSM), conventional nipple-sparing mastectomy (CNSM), and endoscope-assisted nipple-sparing mastectomy (ENSM), each combined with immediate prosthetic breast reconstruction (IPBR), for the treatment of breast cancer. Relevant studies published up to June 15, 2024, were identified through searches of PubMed, Embase, the Cochrane Library, and Web of Science. Data extracted from these studies were analyzed using Stata 15.1 and the Gemtc 1.0.1 package in R 4.2.3. A Bayesian framework and a Markov Chain Monte Carlo model were employed to conduct the NMA. Additionally, a ranking chart was generated to compare the advantages and disadvantages of the surgical methods. Ten studies met the inclusion criteria and were included in the NMA. The results indicated that ENSM with immediate implant-based reconstruction was associated with a smaller incision compared to CNSM. RNSM combined with IPBR was linked to a lower incidence of total complications, Grade 3 complications, and nipple-areola complex necrosis than CNSM. Furthermore, RNSM with IPBR demonstrated a lower recurrence rate than CNSM. However, CNSM with IPBR showed better outcomes in terms of surgical time, hospital stay, and positive margin infiltration. In contrast, RNSM and ENSM, both combined with IPBR, outperformed CNSM in terms of incision length, complication rates, and recurrence outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


