Effective Management of a Skin and Soft Tissue Infection Caused by Community-Acquired MRSA Through Triple-Targeted Therapy Along with Aggressive Source Control: A Case Report.
{"title":"Effective Management of a Skin and Soft Tissue Infection Caused by Community-Acquired MRSA Through Triple-Targeted Therapy Along with Aggressive Source Control: A Case Report.","authors":"Matteo Laratta, Stefano Agliardi, Matteo Sola, Stefano Spina, Roberto Fumagalli","doi":"10.3390/idr17020027","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Methicillin-resistant <i>Staphylococcus aureus</i> (MRSA) is a significant cause of healthcare-associated infections in Europe. It has become increasingly prevalent in community settings, causing skin and soft tissue infections (SSTIs). Managing community-acquired (CA) MRSA infections is challenging due to its high virulence and resistance to common antibiotics, and prevention outside the hospital setting is complex. Combination therapy has demonstrated efficacy in the treatment of severe MRSA infections. Furthermore, surgical source control is critical in treating CA-MRSA infections, involving removing the primary infection site to interrupt bacterial replication. Timeliness and a correct surgical approach are essential for successful treatment outcomes and improved quality of life. <b>Methods:</b> This report details the case of a 15-year-old athlete who was admitted to the intensive care unit with septic shock caused by CA-MRSA. <b>Results:</b> Despite initial treatment, his condition rapidly worsened. A computed tomography (CT) scan identified multiple abscesses (in the lungs, limbs, thyroid, and subscapular region) along with other complications. To achieve adequate tissue concentrations at all affected sites, a triple-targeted antimicrobial therapy was initiated and adjusted based on therapeutic drug monitoring (TDM). At the same time, daily surgical debridement was performed. The patient responded significantly to this treatment, and blood cultures eventually returned negative. <b>Conclusions:</b> A multidisciplinary approach involving early source control, tailored antimicrobial therapy, and, if monotherapy fails to control infection, combination therapy is advisable to treat life-threatening CA-MRSA infections.</p>","PeriodicalId":13579,"journal":{"name":"Infectious Disease Reports","volume":"17 2","pages":""},"PeriodicalIF":2.4000,"publicationDate":"2025-03-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12026867/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious Disease Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/idr17020027","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
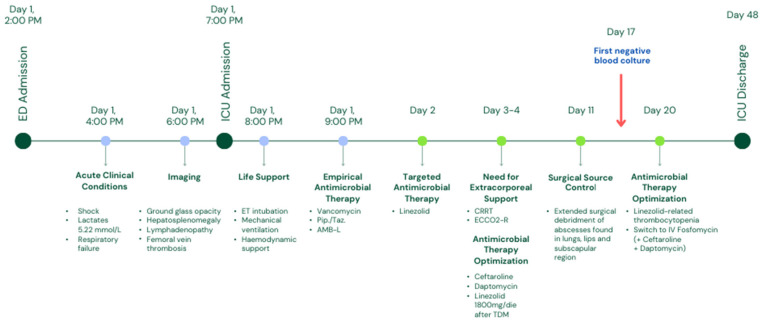
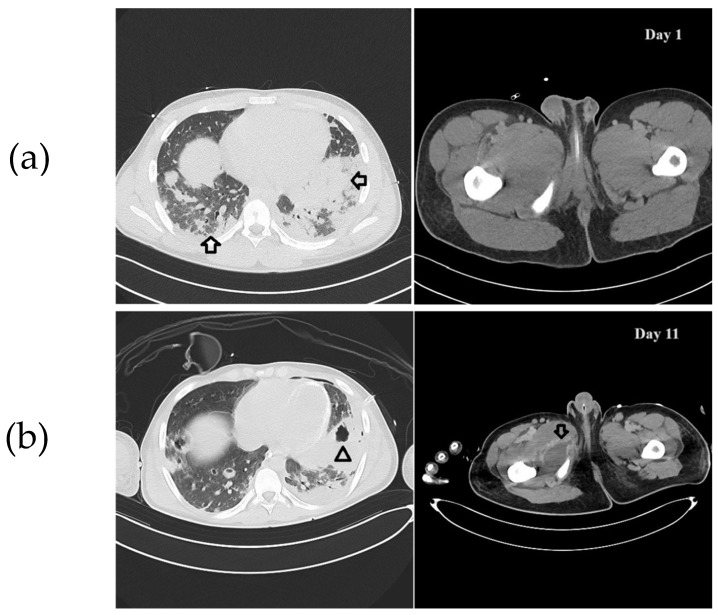
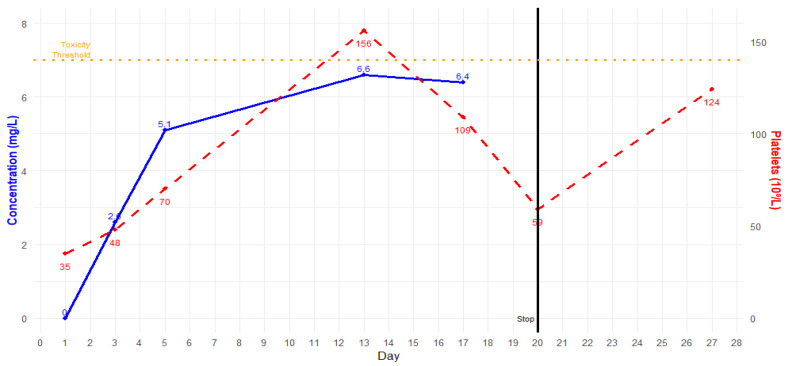
Background: Methicillin-resistant Staphylococcus aureus (MRSA) is a significant cause of healthcare-associated infections in Europe. It has become increasingly prevalent in community settings, causing skin and soft tissue infections (SSTIs). Managing community-acquired (CA) MRSA infections is challenging due to its high virulence and resistance to common antibiotics, and prevention outside the hospital setting is complex. Combination therapy has demonstrated efficacy in the treatment of severe MRSA infections. Furthermore, surgical source control is critical in treating CA-MRSA infections, involving removing the primary infection site to interrupt bacterial replication. Timeliness and a correct surgical approach are essential for successful treatment outcomes and improved quality of life. Methods: This report details the case of a 15-year-old athlete who was admitted to the intensive care unit with septic shock caused by CA-MRSA. Results: Despite initial treatment, his condition rapidly worsened. A computed tomography (CT) scan identified multiple abscesses (in the lungs, limbs, thyroid, and subscapular region) along with other complications. To achieve adequate tissue concentrations at all affected sites, a triple-targeted antimicrobial therapy was initiated and adjusted based on therapeutic drug monitoring (TDM). At the same time, daily surgical debridement was performed. The patient responded significantly to this treatment, and blood cultures eventually returned negative. Conclusions: A multidisciplinary approach involving early source control, tailored antimicrobial therapy, and, if monotherapy fails to control infection, combination therapy is advisable to treat life-threatening CA-MRSA infections.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


