Weilin Song, Adrian Au, David Sarraf, Pradeep Prasad, Edmund Tsui
{"title":"Bilateral acute multifocal retinitis and retinal vasculitis secondary to Rickettsia typhi infection.","authors":"Weilin Song, Adrian Au, David Sarraf, Pradeep Prasad, Edmund Tsui","doi":"10.1186/s12348-025-00496-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To describe a case of acute multifocal retinitis (AMR) and retinal vasculitis associated with Rickettsia typhi.</p><p><strong>Methods: </strong>Case report.</p><p><strong>Results: </strong>A 37-year-old previously healthy female presented with acute bilateral panuveitis that was preceded by a febrile illness with pneumonitis and transaminitis. On exam she had bilateral multifocal small white retinal lesions, vascular sheathing, and hemorrhages. The retinal lesions, which appeared consistent with infiltrates and/or ischemia, were confined within the inner or middle retinal layers on optical coherence tomography (OCT) and corresponded to late leakage on fluorescein angiography (FA). There was no evidence of choroidal involvement on indocyanine green angiography (ICGA). Based on the imaging findings and history, the diagnosis of AMR with associated small vessel retinal vasculitis was made and the patient was started empirically on doxycycline. Workup was positive for R. typhi. At follow-up, there was resolution of visual symptoms and nearly all retinal lesions.</p><p><strong>Conclusions: </strong>Rickettsial disease should be highly suspected in a patient with AMR and occlusive small vessel vasculitis. Retinal lesions may be either infiltrative or ischemic in nature. Diagnosis, which can be aided by multimodal retinal imaging, is essential for prompt initiation of appropriate antibiotic therapy.</p>","PeriodicalId":16600,"journal":{"name":"Journal of Ophthalmic Inflammation and Infection","volume":"15 1","pages":"38"},"PeriodicalIF":2.3000,"publicationDate":"2025-04-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12011691/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Ophthalmic Inflammation and Infection","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s12348-025-00496-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OPHTHALMOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: To describe a case of acute multifocal retinitis (AMR) and retinal vasculitis associated with Rickettsia typhi.
Methods: Case report.
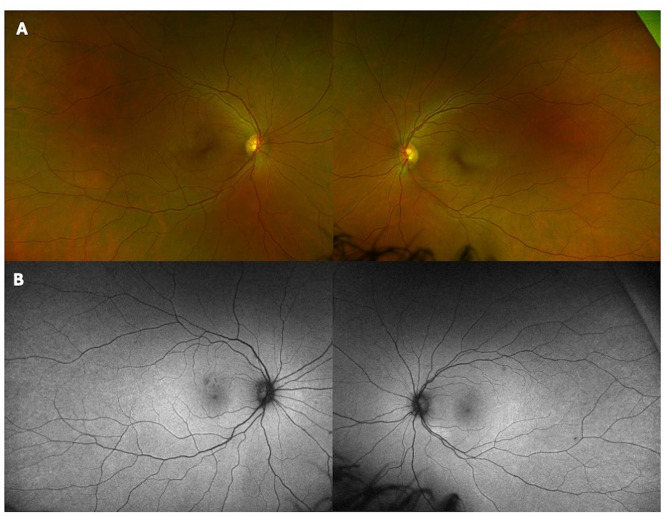
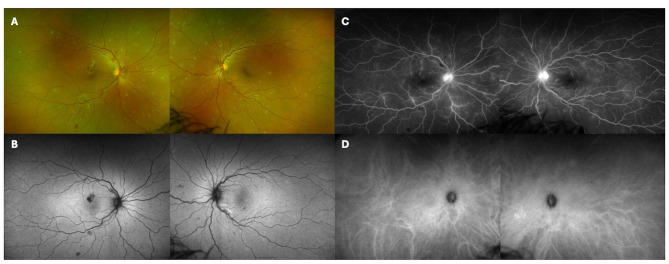
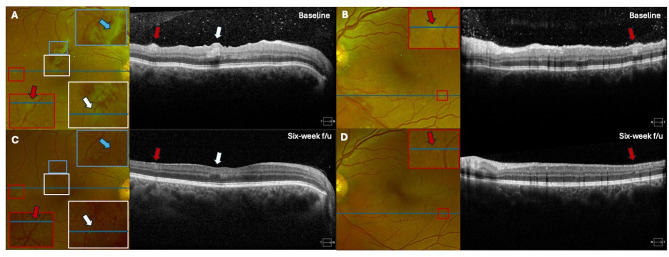
Results: A 37-year-old previously healthy female presented with acute bilateral panuveitis that was preceded by a febrile illness with pneumonitis and transaminitis. On exam she had bilateral multifocal small white retinal lesions, vascular sheathing, and hemorrhages. The retinal lesions, which appeared consistent with infiltrates and/or ischemia, were confined within the inner or middle retinal layers on optical coherence tomography (OCT) and corresponded to late leakage on fluorescein angiography (FA). There was no evidence of choroidal involvement on indocyanine green angiography (ICGA). Based on the imaging findings and history, the diagnosis of AMR with associated small vessel retinal vasculitis was made and the patient was started empirically on doxycycline. Workup was positive for R. typhi. At follow-up, there was resolution of visual symptoms and nearly all retinal lesions.
Conclusions: Rickettsial disease should be highly suspected in a patient with AMR and occlusive small vessel vasculitis. Retinal lesions may be either infiltrative or ischemic in nature. Diagnosis, which can be aided by multimodal retinal imaging, is essential for prompt initiation of appropriate antibiotic therapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


