Grace R Fassina, Emily E Nguyen, David Cho, Drake J Williams, Alexander R Evans, Panayiotis E Pelargos, Christopher S Graffeo
{"title":"The Question Mark Question: Wound Healing after Hemicraniectomy.","authors":"Grace R Fassina, Emily E Nguyen, David Cho, Drake J Williams, Alexander R Evans, Panayiotis E Pelargos, Christopher S Graffeo","doi":"10.1055/a-2561-7951","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The reverse question mark (RQM) incision is the conventional scalp flap technique incorporated during decompressive hemicraniectomy (DHC) operations. Recently, the retroauricular (RA) incision emerged as a possible alternative. We sought to assess the contemporary literature regarding postoperative outcomes following RQM or RA for DHC and subsequent cranioplasty.</p><p><strong>Methods: </strong>MEDLINE and Embase databases were queried using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Studies reporting outcomes after primary DHC and secondary cranioplasty for both RQM and RA were included in a meta-analysis of proportions performed using random-effects modeling.</p><p><strong>Results: </strong>Five manuscripts representing a total of 511 patients met the inclusion criteria. No difference was observed in the rate of primary surgical site infection (SSI) after RQM as compared with RA (OR = 1.64, 95% CI = 0.92-2.92). Similarly, based on those four studies reporting SSI data after cranioplasty, no difference was detected in secondary SSI rates between RQM and RA (OR = 1.93, 95% CI = 0.79-4.72). Patients who underwent primary RQM had increased odds of undergoing cranioplasty compared with patients who had received a primary RA (OR = 1.57, 95% CI = 1.03-2.39).</p><p><strong>Conclusion: </strong>This novel systematic review and meta-analysis reported postoperative outcomes after DHC using either the RQM or RA incision technique. No significant difference was noted in SSI after either the primary decompression or the secondary cranioplasty. These findings support the use of either technique in routine practice, as guided by surgeon preference or other clinical considerations, such as superficial temporal artery preservation for an unrelated future indication.</p>","PeriodicalId":44256,"journal":{"name":"Journal of Neurological Surgery Reports","volume":"86 2","pages":"e77-e82"},"PeriodicalIF":0.7000,"publicationDate":"2025-04-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12020538/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neurological Surgery Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-2561-7951","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
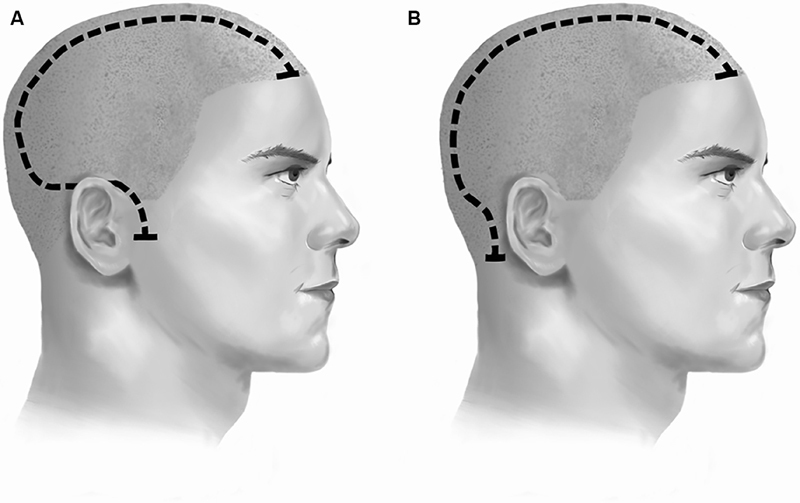
Introduction: The reverse question mark (RQM) incision is the conventional scalp flap technique incorporated during decompressive hemicraniectomy (DHC) operations. Recently, the retroauricular (RA) incision emerged as a possible alternative. We sought to assess the contemporary literature regarding postoperative outcomes following RQM or RA for DHC and subsequent cranioplasty.
Methods: MEDLINE and Embase databases were queried using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Studies reporting outcomes after primary DHC and secondary cranioplasty for both RQM and RA were included in a meta-analysis of proportions performed using random-effects modeling.
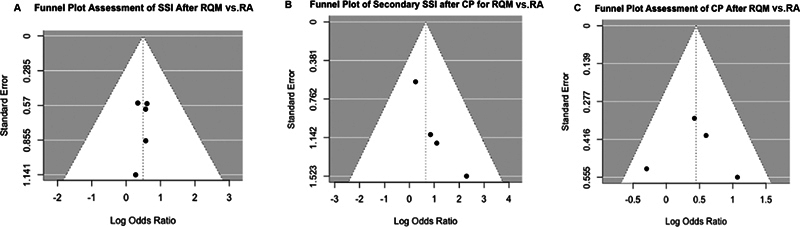
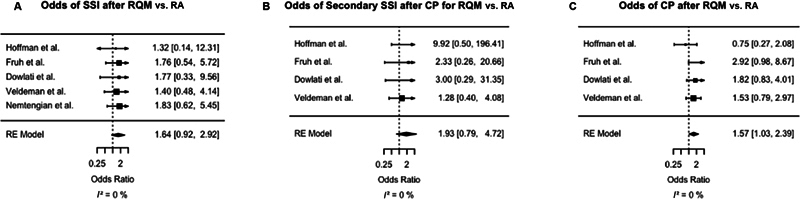
Results: Five manuscripts representing a total of 511 patients met the inclusion criteria. No difference was observed in the rate of primary surgical site infection (SSI) after RQM as compared with RA (OR = 1.64, 95% CI = 0.92-2.92). Similarly, based on those four studies reporting SSI data after cranioplasty, no difference was detected in secondary SSI rates between RQM and RA (OR = 1.93, 95% CI = 0.79-4.72). Patients who underwent primary RQM had increased odds of undergoing cranioplasty compared with patients who had received a primary RA (OR = 1.57, 95% CI = 1.03-2.39).
Conclusion: This novel systematic review and meta-analysis reported postoperative outcomes after DHC using either the RQM or RA incision technique. No significant difference was noted in SSI after either the primary decompression or the secondary cranioplasty. These findings support the use of either technique in routine practice, as guided by surgeon preference or other clinical considerations, such as superficial temporal artery preservation for an unrelated future indication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


