A critical appraisal of the clinico-radiological, histopathological and immunohistochemical profile of CT-guided and bronchoscopy-guided biopsies in lung lesions.
{"title":"A critical appraisal of the clinico-radiological, histopathological and immunohistochemical profile of CT-guided and bronchoscopy-guided biopsies in lung lesions.","authors":"Mukta Pujani, Ruchi Arora Sachdeva, S Zafar Abbas, Charu Agarwal, Minakshi Bhardwaj, Varsha Chauhan, Jyoti Rajpoot, Dipti Sidam, Aniruna Dey","doi":"10.4103/lungindia.lungindia_496_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Lung biopsies are obtained by bronchoscopy or by percutaneous route under image guidance and usually have limited tissue material. It is quite challenging for a pathologist to make an accurate diagnosis of lung cancer using only a limited panel of immunohistochemical markers and mucin stains as well as spare as much tissue for molecular testing.Molecular testing for specific genetic mutations or biomarkers serves as an adjunct for more rational, targeted treatment regimens.</p><p><strong>Methods: </strong>All the consecutive image-guided lung biopsies (both computed tomography [CT] guided and bronchoscopy-guided) for a period of 3 years (2021-2024) were included in the study. The clinicopathological data was compiled from the hospital records, and histopathology and immunohistochemistry (IHC) were analysed critically for all lung carcinomas. Sensitivity, specificity, negative predictive value, positive predictive value and diagnostic accuracy were calculated for IHC markers.</p><p><strong>Results: </strong>There were 127 lung biopsies (117 bronchoscopic and 10 CT-guided biopsies) comprise of adenocarcinoma (30%), squamous cell carcinoma (25.2%), small-cell carcinoma (13.4%) and poorly differentiated carcinoma (6.3%). The concordance between clinico-radiological and pathological diagnosis was 85%. P40 (22/22 cases) and CK5/6 (10/10) were the most sensitive and specific markers for squamous cell carcinoma, while TTF-1 (35/36) and Napsin A (18/22) were the most sensitive IHC markers for adenocarcinoma. The most sensitive markers for small-cell carcinoma lung were synaptophysin (17/17), CD 56, NSE followed by chromogranin A (11/15).</p><p><strong>Conclusion: </strong>Integrating conventional histopathology with IHC results in accurate diagnosis, thereby avoiding a broad diagnosis of non-small-cell lung carcinoma (NSCLC). Subclassification of NSCLC has significant treatment implications, especially for advanced-stage tumours for which chemotherapy or targeted therapy is being considered. The focus should be on the judicious use of IHC based on histological type because of the limited availability of tissues in bronchoscopic and CT-guided biopsy specimens.</p>","PeriodicalId":47462,"journal":{"name":"Lung India","volume":"42 3","pages":"218-224"},"PeriodicalIF":1.2000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12097671/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Lung India","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/lungindia.lungindia_496_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/29 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Lung biopsies are obtained by bronchoscopy or by percutaneous route under image guidance and usually have limited tissue material. It is quite challenging for a pathologist to make an accurate diagnosis of lung cancer using only a limited panel of immunohistochemical markers and mucin stains as well as spare as much tissue for molecular testing.Molecular testing for specific genetic mutations or biomarkers serves as an adjunct for more rational, targeted treatment regimens.
Methods: All the consecutive image-guided lung biopsies (both computed tomography [CT] guided and bronchoscopy-guided) for a period of 3 years (2021-2024) were included in the study. The clinicopathological data was compiled from the hospital records, and histopathology and immunohistochemistry (IHC) were analysed critically for all lung carcinomas. Sensitivity, specificity, negative predictive value, positive predictive value and diagnostic accuracy were calculated for IHC markers.
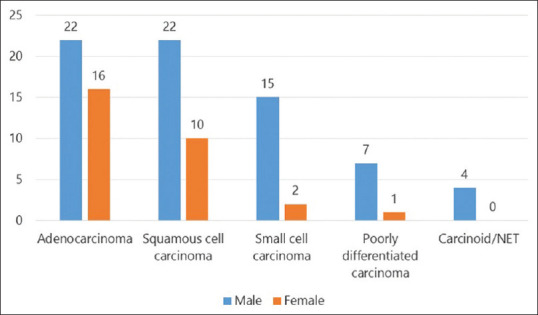
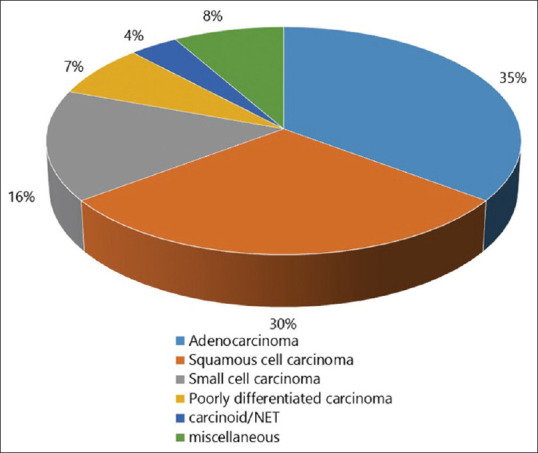
Results: There were 127 lung biopsies (117 bronchoscopic and 10 CT-guided biopsies) comprise of adenocarcinoma (30%), squamous cell carcinoma (25.2%), small-cell carcinoma (13.4%) and poorly differentiated carcinoma (6.3%). The concordance between clinico-radiological and pathological diagnosis was 85%. P40 (22/22 cases) and CK5/6 (10/10) were the most sensitive and specific markers for squamous cell carcinoma, while TTF-1 (35/36) and Napsin A (18/22) were the most sensitive IHC markers for adenocarcinoma. The most sensitive markers for small-cell carcinoma lung were synaptophysin (17/17), CD 56, NSE followed by chromogranin A (11/15).
Conclusion: Integrating conventional histopathology with IHC results in accurate diagnosis, thereby avoiding a broad diagnosis of non-small-cell lung carcinoma (NSCLC). Subclassification of NSCLC has significant treatment implications, especially for advanced-stage tumours for which chemotherapy or targeted therapy is being considered. The focus should be on the judicious use of IHC based on histological type because of the limited availability of tissues in bronchoscopic and CT-guided biopsy specimens.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


