Anne A C van Tetering, Ella L de Vries, Peter Ntuyo, E R van den Heuvel, Annemarie F Fransen, M Beatrijs van der Hout-van der Jagt, Imelda Namagembe, Josaphat Byamugisha, S Guid Oei
{"title":"Mono-Professional Simulation-Based Obstetric Training in a Low-Resource Setting: Stepped-Wedge Cluster Randomized Trial.","authors":"Anne A C van Tetering, Ella L de Vries, Peter Ntuyo, E R van den Heuvel, Annemarie F Fransen, M Beatrijs van der Hout-van der Jagt, Imelda Namagembe, Josaphat Byamugisha, S Guid Oei","doi":"10.2196/54911","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Emergency obstetric simulation-based training has increasingly been used to improve emergency obstetric care provision in sub-Saharan Africa. For determining the optimal methodology for effective training sessions in resource-constrained settings, it is crucial to conduct high-quality research.</p><p><strong>Objective: </strong>We aim to investigate the impact of a train-the-trainer model for providing technology-enhanced, mono-professional, simulation-based training in obstetrics in a resource-constrained setting on maternal and perinatal outcomes.</p><p><strong>Methods: </strong>A stepped-wedge cluster randomized trial was conducted from October 2014 until March 2016 at the medium- to high-risk ward at Mulago National Referral Hospital, Uganda, with an annual delivery rate of over 23,000. The intervention consisted of a train-the-trainer model in which training was cascaded down from master trainers to local facilitators (obstetric senior staff members) to learners (senior house officers). The training of senior house officers was provided to 7 fixed clusters by a computer-generated random sequential roll-out. The training comprised a 1-day (8 h), mono-professional, simulation-based training in obstetrics, and half-day repetition training sessions targeted at every 7 weeks. Both medical technical skills and teamwork skills were taught. The primary outcome comprised a combined maternal and perinatal mortality rate. Secondary outcomes comprised the maternal mortality rate, the perinatal mortality rate, the percentage of births by vacuum extraction and cesarean section, and the Weighted Adverse Outcome Score.</p><p><strong>Results: </strong>Overall, there were 17,496 births. The combined mortality rate was 9.05% (95% CI 8.37%-9.77%) in the intervention group, and 8.73% (95% CI 8.21%-9.28%) in the control group (odds ratio [OR] 0.98, 95% CI 0.86-1.12; P=.81). No statistically significant change was found in the maternal mortality rate (OR 0.80, 95% CI 0.27-2.32; P=.68) or the perinatal mortality rate (OR 0.99, 95% CI 0.87-1.13; P=.87). This study did not identify any difference in the percentage of vacuum extractions, the percentage of cesarean sections, or Weighted Adverse Outcome Scores.</p><p><strong>Conclusions: </strong>This train-the-trainer model for providing technology-enhanced, mono-professional, simulation-based training in obstetrics was not able to change maternal and perinatal mortality outcomes. This study, in combination with literature, suggests that future research should consider multiprofessional team training in obstetrics involving all staff within their units.</p>","PeriodicalId":36236,"journal":{"name":"JMIR Medical Education","volume":"11 ","pages":"e54911"},"PeriodicalIF":3.2000,"publicationDate":"2025-05-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12083734/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR Medical Education","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/54911","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EDUCATION, SCIENTIFIC DISCIPLINES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Emergency obstetric simulation-based training has increasingly been used to improve emergency obstetric care provision in sub-Saharan Africa. For determining the optimal methodology for effective training sessions in resource-constrained settings, it is crucial to conduct high-quality research.
Objective: We aim to investigate the impact of a train-the-trainer model for providing technology-enhanced, mono-professional, simulation-based training in obstetrics in a resource-constrained setting on maternal and perinatal outcomes.
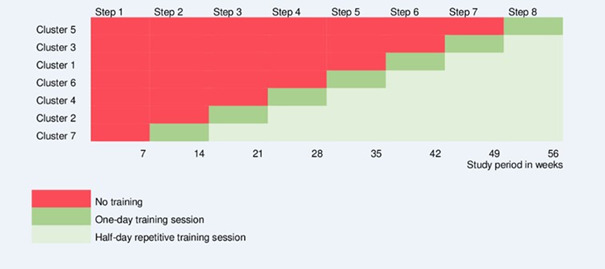
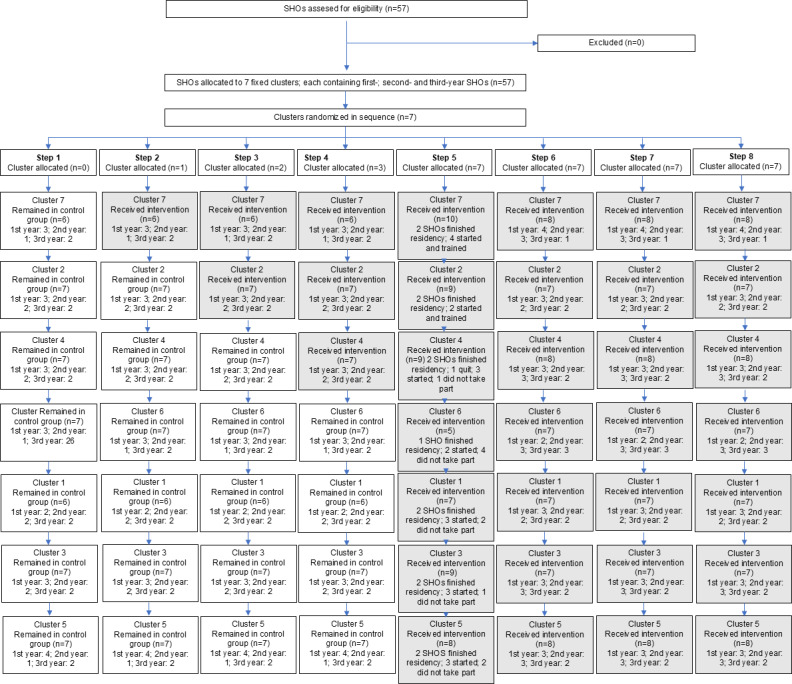
Methods: A stepped-wedge cluster randomized trial was conducted from October 2014 until March 2016 at the medium- to high-risk ward at Mulago National Referral Hospital, Uganda, with an annual delivery rate of over 23,000. The intervention consisted of a train-the-trainer model in which training was cascaded down from master trainers to local facilitators (obstetric senior staff members) to learners (senior house officers). The training of senior house officers was provided to 7 fixed clusters by a computer-generated random sequential roll-out. The training comprised a 1-day (8 h), mono-professional, simulation-based training in obstetrics, and half-day repetition training sessions targeted at every 7 weeks. Both medical technical skills and teamwork skills were taught. The primary outcome comprised a combined maternal and perinatal mortality rate. Secondary outcomes comprised the maternal mortality rate, the perinatal mortality rate, the percentage of births by vacuum extraction and cesarean section, and the Weighted Adverse Outcome Score.
Results: Overall, there were 17,496 births. The combined mortality rate was 9.05% (95% CI 8.37%-9.77%) in the intervention group, and 8.73% (95% CI 8.21%-9.28%) in the control group (odds ratio [OR] 0.98, 95% CI 0.86-1.12; P=.81). No statistically significant change was found in the maternal mortality rate (OR 0.80, 95% CI 0.27-2.32; P=.68) or the perinatal mortality rate (OR 0.99, 95% CI 0.87-1.13; P=.87). This study did not identify any difference in the percentage of vacuum extractions, the percentage of cesarean sections, or Weighted Adverse Outcome Scores.
Conclusions: This train-the-trainer model for providing technology-enhanced, mono-professional, simulation-based training in obstetrics was not able to change maternal and perinatal mortality outcomes. This study, in combination with literature, suggests that future research should consider multiprofessional team training in obstetrics involving all staff within their units.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


