{"title":"[Time of entry into care of people living with HIV in two outpatient treatment centers of Libreville, Gabon, between 2012 and 2020].","authors":"Michèle Marion Ntsame Owono, Magalie Essomeyo Ngue Mebale, Charleine Manomba Boulingui, Bridy Moutombi Ditombi, Philomène Kouna Ndouongo, Marielle Karine Bouyou Akotet","doi":"10.48327/mtsi.v5i1.2025.537","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Delays in entry to care are a barrier to immediate initiation of antiretroviral therapy (ART) at diagnosis, as recommended by the World Health Organization. The aim of this study was to determine and compare delays in entry into care and associated factors among people living with HIV (PLHIV) seen at two outpatient treatment centers in Libreville between 2012 and 2020.</p><p><strong>Materials and methods: </strong>Retrospective study based on PLHIV records collected from January 2012 to March 2020 at the two largest outpatient treatment centers (CTA) in Libreville, that of the Centre Hospitalier Universitaire de Libreville (CHUL) and that of Nkembo Hospital. Early entry into care was defined as less than 28 days between diagnosis of HIV infection and first consultation at the CTA. Late entry was defined as more than three months. For analysis, patients were divided into two periods: 2012-2015, when treatment initiation was linked to CD4 count, and 2016-2020, the period when the <i>Test and Treat</i> method was introduced in Gabon.</p><p><strong>Results: </strong>A total of 979 patients were newly treated in the two CTAs, and the records of 672 individuals could be used. In 48.3% of the cases, HIV infection was diagnosed at a late stage (WHO 3 or 4). The median time to entry into care was 1.2 [IQ: 0-3] months after diagnosis of HIV infection. Between 2016 and 2020, 47% entered care in less than 28 days, compared with 35.7% in 2012-2015 (p < 0.01). The percentage of PLHIV with late entry into care was comparable between the two periods (14.4% vs. 15.9% in 2012-2015; p = 0.62). Factors associated with late entry were WHO stage 3, failure to achieve CD4 count, employment, and pregnancy (p<0.05).</p><p><strong>Conclusion: </strong>In the era of <i>Test and Treat</i> in Libreville, the delay in seeking care is still long. A better understanding of the associated factors and a decentralized, integrated approach to the management of HIV infection would make it possible to achieve the second pillar of \"95-95-95\" target in Libreville.</p>","PeriodicalId":101416,"journal":{"name":"Medecine tropicale et sante internationale","volume":"5 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-02-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12001990/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medecine tropicale et sante internationale","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.48327/mtsi.v5i1.2025.537","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/31 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Delays in entry to care are a barrier to immediate initiation of antiretroviral therapy (ART) at diagnosis, as recommended by the World Health Organization. The aim of this study was to determine and compare delays in entry into care and associated factors among people living with HIV (PLHIV) seen at two outpatient treatment centers in Libreville between 2012 and 2020.
Materials and methods: Retrospective study based on PLHIV records collected from January 2012 to March 2020 at the two largest outpatient treatment centers (CTA) in Libreville, that of the Centre Hospitalier Universitaire de Libreville (CHUL) and that of Nkembo Hospital. Early entry into care was defined as less than 28 days between diagnosis of HIV infection and first consultation at the CTA. Late entry was defined as more than three months. For analysis, patients were divided into two periods: 2012-2015, when treatment initiation was linked to CD4 count, and 2016-2020, the period when the Test and Treat method was introduced in Gabon.
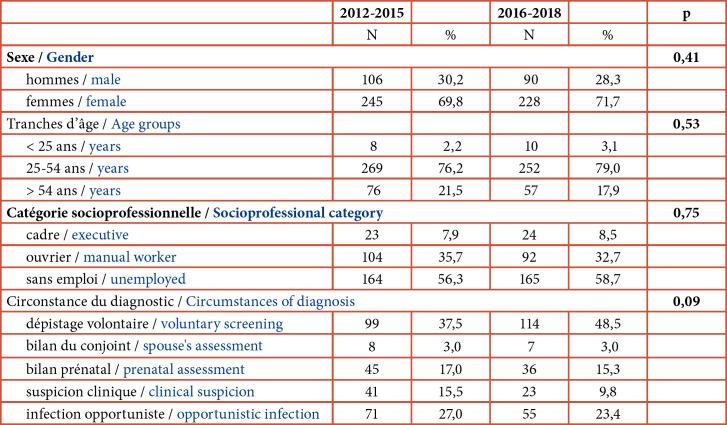
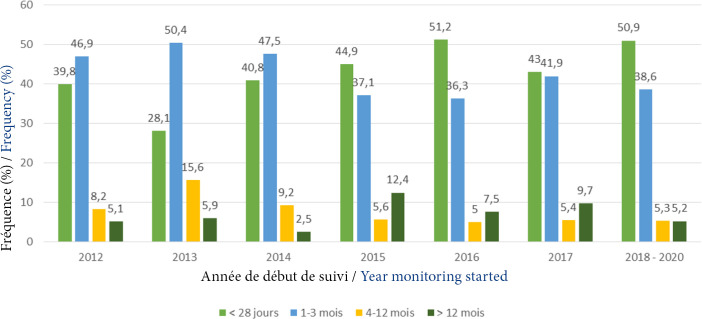
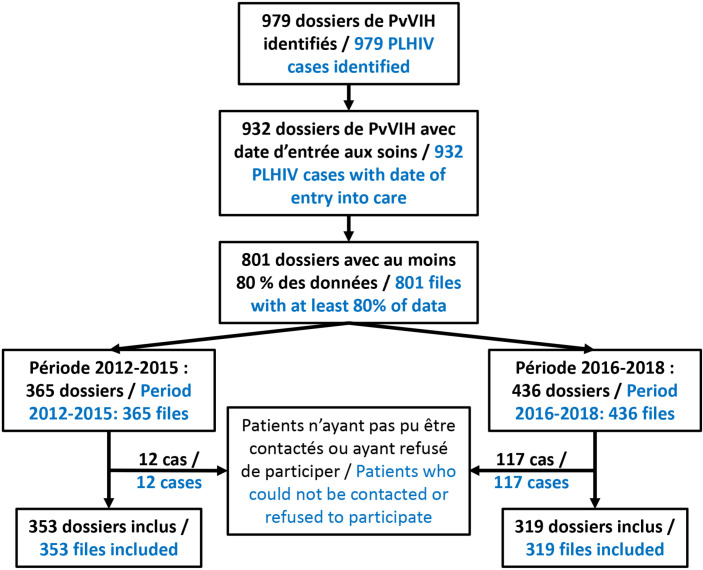
Results: A total of 979 patients were newly treated in the two CTAs, and the records of 672 individuals could be used. In 48.3% of the cases, HIV infection was diagnosed at a late stage (WHO 3 or 4). The median time to entry into care was 1.2 [IQ: 0-3] months after diagnosis of HIV infection. Between 2016 and 2020, 47% entered care in less than 28 days, compared with 35.7% in 2012-2015 (p < 0.01). The percentage of PLHIV with late entry into care was comparable between the two periods (14.4% vs. 15.9% in 2012-2015; p = 0.62). Factors associated with late entry were WHO stage 3, failure to achieve CD4 count, employment, and pregnancy (p<0.05).
Conclusion: In the era of Test and Treat in Libreville, the delay in seeking care is still long. A better understanding of the associated factors and a decentralized, integrated approach to the management of HIV infection would make it possible to achieve the second pillar of "95-95-95" target in Libreville.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


