Association of Adjunctive Procedures, Patient Demographics, or Intraoperative Factors and the Risk of Complications or Reoperation Following Total Ankle Arthroplasty or Ankle Arthrodesis.
Ramiro Lopez, Cole Herbel, Glenn G Shi, Edward T Haupt
{"title":"Association of Adjunctive Procedures, Patient Demographics, or Intraoperative Factors and the Risk of Complications or Reoperation Following Total Ankle Arthroplasty or Ankle Arthrodesis.","authors":"Ramiro Lopez, Cole Herbel, Glenn G Shi, Edward T Haupt","doi":"10.1177/24730114251329051","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>End-stage ankle arthritis is successfully treated with surgery with either ankle arthrodesis (AA) or total ankle arthroplasty (TAA). Much is described comparing the 2 treatments in tightly selected patient groups. Limited evidence attempts to examine specific elements of technical complexity that increase perioperative risk for the surgical treatment of ankle arthritis. There is suspicion that AA may be preferable in the setting of elevated patient complexity, or that procedures may require staging to diminish complication risk when there is also foot deformity present. The aim of this study is to evaluate the effect of adjunctive procedures on overall postoperative complication (POC) risk, for both TAA and AA. Primary outcome measures were to compare overall complication and reoperation risk for TAA and AA. Secondary outcome measures were to identify patient factors, intraoperative factors, and factors of procedural complexity via number of associated surgeries and the incidence of complications and reoperation.</p><p><strong>Methods: </strong>A retrospective chart review of AAs and TAAs performed at a single academic institution from the years 2008-2024 was performed using <i>Current Procedural Terminology</i> (<i>CPT</i>) codes identifying AA and TAA. Patient demographics, operative details, and postoperative data were abstracted to collect relevant information. Statistical analyses, including odds ratios and analysis of variance, were then performed to reveal specific risk factors and correlations.</p><p><strong>Results: </strong>Four hundred ninety-one patients were identified in the initial database query. After exclusions, 246 remained, of which 110 underwent AA and 136 underwent TAA. The mean length of follow-up was 36.4 months for TAA patients and 46.1 months for AA patients in this study. Overall, patients who underwent TAA were older and had an increased number of preoperative comorbidities (5.74 ± 3.07) compared to AA (4.74 ± 2.76) (<i>P</i> = .008). Additionally, TAA patients experienced a lower overall rate of POCs (20/136, 14.71%) and reoperation (14/136, 10.29%) compared with patients who underwent AA (21/110, 19.09%; 21/110, 19.09%) (<i>P</i> = .36 and <i>P</i> = .05, respectively). As the number of adjunctive procedures increased, so did the rate of POCs, but not reoperation, in patients who underwent TAA. The number of adjunctive procedures was not significantly associated with complication or reoperation risk in AA patients. There were no specific adjunctive procedures that demonstrated a significant correlation with increased risk of complications or reoperation in both groups. Osteoporosis and coagulopathies were identified as predisposing TAA patients to postoperative complications.</p><p><strong>Conclusion: </strong>In our retrospective cohort study with relatively low statistical power, we found that patients who undergo TAA or AA plus adjunctive procedures did not experience an increased risk of major complications or reoperation compared to patients who did not undergo adjunctive procedures. Several preexisting comorbidities in TAA patients were associated with higher rates of POCs or reoperation, including osteoporosis and coagulopathies; no comorbidities were linked to increased reoperation or POC risk in the AA group. These findings suggest a need to evaluate comorbidities, and lifestyle factors when recommending an ankle reconstruction procedure to minimize the odds of postoperative complications and improve likelihood of patient satisfaction.</p><p><strong>Level of evidence: </strong>Level III, retrospective cohort study.</p>","PeriodicalId":12429,"journal":{"name":"Foot & Ankle Orthopaedics","volume":"10 2","pages":"24730114251329051"},"PeriodicalIF":0.0000,"publicationDate":"2025-04-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12034974/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Foot & Ankle Orthopaedics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/24730114251329051","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: End-stage ankle arthritis is successfully treated with surgery with either ankle arthrodesis (AA) or total ankle arthroplasty (TAA). Much is described comparing the 2 treatments in tightly selected patient groups. Limited evidence attempts to examine specific elements of technical complexity that increase perioperative risk for the surgical treatment of ankle arthritis. There is suspicion that AA may be preferable in the setting of elevated patient complexity, or that procedures may require staging to diminish complication risk when there is also foot deformity present. The aim of this study is to evaluate the effect of adjunctive procedures on overall postoperative complication (POC) risk, for both TAA and AA. Primary outcome measures were to compare overall complication and reoperation risk for TAA and AA. Secondary outcome measures were to identify patient factors, intraoperative factors, and factors of procedural complexity via number of associated surgeries and the incidence of complications and reoperation.
Methods: A retrospective chart review of AAs and TAAs performed at a single academic institution from the years 2008-2024 was performed using Current Procedural Terminology (CPT) codes identifying AA and TAA. Patient demographics, operative details, and postoperative data were abstracted to collect relevant information. Statistical analyses, including odds ratios and analysis of variance, were then performed to reveal specific risk factors and correlations.
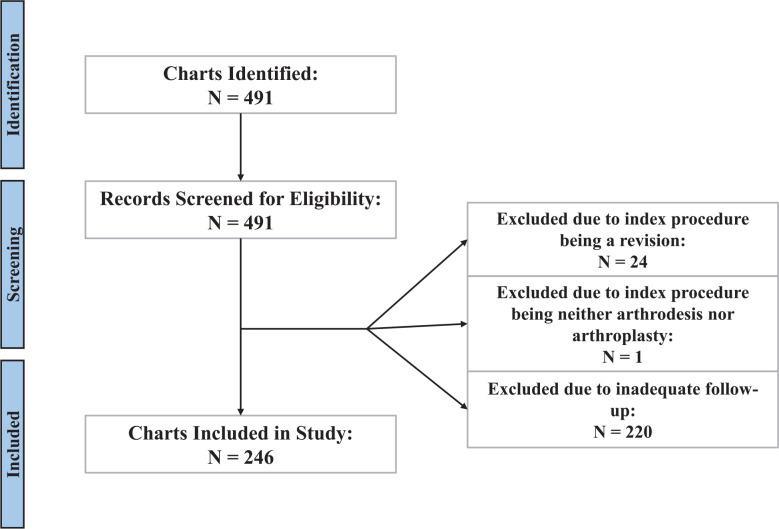
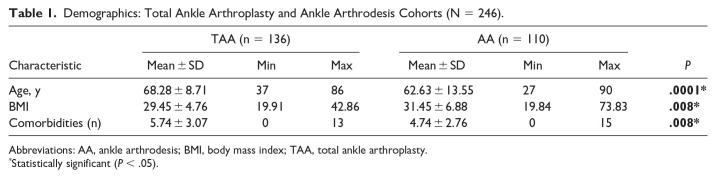
Results: Four hundred ninety-one patients were identified in the initial database query. After exclusions, 246 remained, of which 110 underwent AA and 136 underwent TAA. The mean length of follow-up was 36.4 months for TAA patients and 46.1 months for AA patients in this study. Overall, patients who underwent TAA were older and had an increased number of preoperative comorbidities (5.74 ± 3.07) compared to AA (4.74 ± 2.76) (P = .008). Additionally, TAA patients experienced a lower overall rate of POCs (20/136, 14.71%) and reoperation (14/136, 10.29%) compared with patients who underwent AA (21/110, 19.09%; 21/110, 19.09%) (P = .36 and P = .05, respectively). As the number of adjunctive procedures increased, so did the rate of POCs, but not reoperation, in patients who underwent TAA. The number of adjunctive procedures was not significantly associated with complication or reoperation risk in AA patients. There were no specific adjunctive procedures that demonstrated a significant correlation with increased risk of complications or reoperation in both groups. Osteoporosis and coagulopathies were identified as predisposing TAA patients to postoperative complications.
Conclusion: In our retrospective cohort study with relatively low statistical power, we found that patients who undergo TAA or AA plus adjunctive procedures did not experience an increased risk of major complications or reoperation compared to patients who did not undergo adjunctive procedures. Several preexisting comorbidities in TAA patients were associated with higher rates of POCs or reoperation, including osteoporosis and coagulopathies; no comorbidities were linked to increased reoperation or POC risk in the AA group. These findings suggest a need to evaluate comorbidities, and lifestyle factors when recommending an ankle reconstruction procedure to minimize the odds of postoperative complications and improve likelihood of patient satisfaction.
Level of evidence: Level III, retrospective cohort study.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


