Improved Sixty-Day Mortality in Candidemia with Antifungal Treatment Within 72 Hours of Fever Onset: A Single-Center Retrospective Study in Rural Japan.
{"title":"Improved Sixty-Day Mortality in Candidemia with Antifungal Treatment Within 72 Hours of Fever Onset: A Single-Center Retrospective Study in Rural Japan.","authors":"Koji Hayashi, Chizuru Hashimoto, Kohei Ueda, Yuka Nakaya, Asuka Suzuki, Maho Hayashi, Mamiko Sato, Yasutaka Kobayashi","doi":"10.3390/idr17020036","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction:</b> Prognostic factor investigations for candidemia have been conducted in large-scale facilities, leading to significant evidence, including early administration of echinocandin antifungal agents and removal of central venous catheters (CVCs). In departments that provide aggressive chemotherapy or transplantation, candidiasis markers are regularly evaluated, and preemptive treatments may be initiated. However, in resource-limited facilities, candidemia detection largely relies on vital signs like fever and blood cultures. This study assessed whether evidence from large-scale facilities applies to such settings. Additionally, while prior studies indicate that early antifungal treatment is based on positive blood cultures, no established criteria exist for early administration based on fever as an indicator. <b>Methods:</b> This study analyzed cases of candidemia from blood cultures at Fukui General Hospital (2014-2024). Patients aged 18 or older with at least one positive blood culture for <i>Candida</i> species and clinical signs of infection were included, while contamination cases were excluded. The patients were categorized into survival and death groups based on 60-day survival from fever onset. The variables collected included age, gender, duration from admission to fever onset, time from fever onset to blood culture collection and antifungal treatment initiation, antifungal treatment within 72 h, serum albumin levels, history of cancer, diabetes, empiric echinocandin treatment, CVC insertion, duration of CVC insertion until fever onset, use of total parenteral nutrition, broad-spectrum antibiotic use, and sequential organ failure assessment (SOFA) score. Fever was defined as a body temperature of 38.0 °C or higher, guiding blood culture collection. <b>Results:</b> Of 30 candidemia cases, 29 were analyzed. Survival was significantly associated with younger age (average 73.3 ± 13.3 vs. 83.1 ± 9.1 years, <i>p</i> = 0.038) and antifungal treatment within 72 h of fever onset (9 vs. 3, <i>p</i> = 0.025). CVC use was of marginal significance (8 vs. 13, <i>p</i> = 0.108). There was a significant difference in the duration (in days) of CVC insertion until fever onset (median [IQR]: 15.5 [11.75-19.5] vs. 30.0 [19.0-39.0], <i>p</i> = 0.027). Logistic regression identified early antifungal treatment (OR = 0.065, <i>p</i> = 0.035) and CVC use (OR = 21.8, <i>p</i> = 0.024) as independent predictors of mortality. <b>Conclusions:</b> Early antifungal treatment within 72 h of fever onset and CVC use were independent predictors of mortality in candidemia. The importance of early antifungal treatment was reaffirmed even in smaller facilities. The impact of CVC insertion on 60-day survival cannot be readily generalized due to the limited sample size. Further research is needed to clarify the impact of fever-based antifungal initiation and CVC use on 60-day survival.</p>","PeriodicalId":13579,"journal":{"name":"Infectious Disease Reports","volume":"17 2","pages":""},"PeriodicalIF":2.4000,"publicationDate":"2025-04-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12027375/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious Disease Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/idr17020036","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
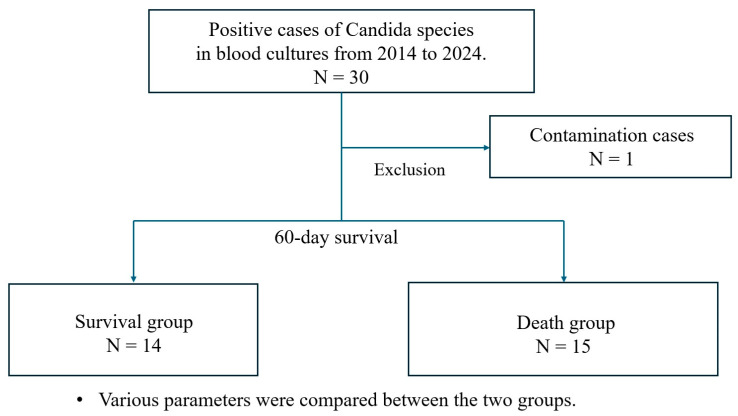
Introduction: Prognostic factor investigations for candidemia have been conducted in large-scale facilities, leading to significant evidence, including early administration of echinocandin antifungal agents and removal of central venous catheters (CVCs). In departments that provide aggressive chemotherapy or transplantation, candidiasis markers are regularly evaluated, and preemptive treatments may be initiated. However, in resource-limited facilities, candidemia detection largely relies on vital signs like fever and blood cultures. This study assessed whether evidence from large-scale facilities applies to such settings. Additionally, while prior studies indicate that early antifungal treatment is based on positive blood cultures, no established criteria exist for early administration based on fever as an indicator. Methods: This study analyzed cases of candidemia from blood cultures at Fukui General Hospital (2014-2024). Patients aged 18 or older with at least one positive blood culture for Candida species and clinical signs of infection were included, while contamination cases were excluded. The patients were categorized into survival and death groups based on 60-day survival from fever onset. The variables collected included age, gender, duration from admission to fever onset, time from fever onset to blood culture collection and antifungal treatment initiation, antifungal treatment within 72 h, serum albumin levels, history of cancer, diabetes, empiric echinocandin treatment, CVC insertion, duration of CVC insertion until fever onset, use of total parenteral nutrition, broad-spectrum antibiotic use, and sequential organ failure assessment (SOFA) score. Fever was defined as a body temperature of 38.0 °C or higher, guiding blood culture collection. Results: Of 30 candidemia cases, 29 were analyzed. Survival was significantly associated with younger age (average 73.3 ± 13.3 vs. 83.1 ± 9.1 years, p = 0.038) and antifungal treatment within 72 h of fever onset (9 vs. 3, p = 0.025). CVC use was of marginal significance (8 vs. 13, p = 0.108). There was a significant difference in the duration (in days) of CVC insertion until fever onset (median [IQR]: 15.5 [11.75-19.5] vs. 30.0 [19.0-39.0], p = 0.027). Logistic regression identified early antifungal treatment (OR = 0.065, p = 0.035) and CVC use (OR = 21.8, p = 0.024) as independent predictors of mortality. Conclusions: Early antifungal treatment within 72 h of fever onset and CVC use were independent predictors of mortality in candidemia. The importance of early antifungal treatment was reaffirmed even in smaller facilities. The impact of CVC insertion on 60-day survival cannot be readily generalized due to the limited sample size. Further research is needed to clarify the impact of fever-based antifungal initiation and CVC use on 60-day survival.
导言:念珠菌病的预后因素调查已经在大型设施中进行,得到了重要的证据,包括早期给药棘白菌素抗真菌药物和去除中心静脉导管(CVCs)。在提供积极化疗或移植的部门,定期评估念珠菌病标志物,并可能开始先发制人的治疗。然而,在资源有限的设施中,念珠菌的检测主要依赖于发烧和血液培养等生命体征。这项研究评估了来自大型设施的证据是否适用于这种情况。此外,虽然先前的研究表明,早期抗真菌治疗是基于阳性血培养,但没有建立的标准,以发烧为指标的早期给药。方法:对2014-2024年福井总医院血培养念珠菌病例进行分析。患者年龄在18岁或以上,且至少有一种念珠菌血培养阳性且有感染临床体征,排除污染病例。根据发热后60天生存率分为生存组和死亡组。收集的变量包括年龄、性别、入院至发热的持续时间、发热至血液培养和开始抗真菌治疗的时间、72h内抗真菌治疗的时间、血清白蛋白水平、癌症史、糖尿病史、经验性棘白菌素治疗、CVC插入、CVC插入至发热的持续时间、全肠外营养的使用、广谱抗生素的使用和序贯器官衰竭评估(SOFA)评分。发热定义为体温38.0°C或更高,指导血液培养采集。结果:30例念珠菌中,分析29例。生存率与年龄较轻(平均73.3±13.3岁比83.1±9.1岁,p = 0.038)和发热72小时内抗真菌治疗显著相关(9比3,p = 0.025)。CVC的使用有边际意义(8 vs. 13, p = 0.108)。CVC插入至发热的持续时间(以天为单位)差异有统计学意义(中位数[IQR]: 15.5 [11.75-19.5] vs. 30.0 [19.0-39.0], p = 0.027)。Logistic回归发现早期抗真菌治疗(OR = 0.065, p = 0.035)和CVC使用(OR = 21.8, p = 0.024)是死亡率的独立预测因子。结论:发热72小时内早期抗真菌治疗和使用CVC是念珠菌病死亡率的独立预测因素。早期抗真菌治疗的重要性即使在较小的设施中也得到了重申。由于样本量有限,CVC植入对60天生存率的影响不能一概而论。需要进一步的研究来阐明基于发热的抗真菌启动和CVC使用对60天生存的影响。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


