Christine Hofmann, Annette Holl-Wieden, Christiane Reiser, Meinrad Beer, Peter Raab, Henner Morbach, Hermann J Girschick
{"title":"Chronic non-bacterial osteomyelitis in children- five-year standardized follow-up of a prospective observational cohort in the pre-biological era.","authors":"Christine Hofmann, Annette Holl-Wieden, Christiane Reiser, Meinrad Beer, Peter Raab, Henner Morbach, Hermann J Girschick","doi":"10.1186/s12969-025-01106-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This prospective, long-term observational study, initiated in 2002, aimed to characterize clinical and laboratory data, whole body MRI detected lesions, and treatment responses in 37 juvenile patients with chronic non-bacterial osteomyelitis at a time when biological DMARDs were not yet standard therapy.</p><p><strong>Methods: </strong>Patients were assessed at baseline and at 1 (without MRI), 3, 6, 12, 18, 24, 36, 48, 60 months. All patients received naproxen as first-line therapy. Clinical management allowed for escalation to sulfasalazine, pamidronate, and glucocorticoids as needed. Treatment response was evaluated using the pedCNO disease activity score (30/50/70/90% improvement). Further composite numeric disease activity (DA) scores- the CARRA CDAS and a new MRI DAS - were applied.</p><p><strong>Results: </strong>The mean age at disease onset was 10.8 years, with a diagnostic delay of 5.8 months. Naproxen was the initial treatment in all patients. Second-line therapy was initiated in 10 patients due to inadequate improvement in physician global assessment of disease activity, patient-reported overall wellbeing or MRI lesions. Escalated therapies included sulfasalazine (n = 10), bisphosphonates (n = 1), methotrexate (n = 1), and short- (< 4 wks) or long-term oral glucocorticoids (n = 5 and n = 3, respectively). The mean number of clinical lesions decreased from 2.1 to 0.4 at 12 months and reached 0.15 at 60 months. MRI-detected lesions declined from 5.0 to 2.25 at 12 months and to 1.1 at 60 months.</p><p><strong>Conclusion: </strong>Most children experienced favourable long-term outcomes. Clinical improvement occurred more rapidly than radiologic resolution. Patients with insufficient response to NSAIDs should be considered for a treat-to-target approach, including the use of conventional and biologic DMARDs.</p><p><strong>Trial registration: </strong>A trial registration EUDRA CT was not available at the time the study was started. Informed consent was given by all parents.</p>","PeriodicalId":54630,"journal":{"name":"Pediatric Rheumatology","volume":"23 1","pages":"50"},"PeriodicalIF":2.3000,"publicationDate":"2025-05-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12076821/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Rheumatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12969-025-01106-2","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: This prospective, long-term observational study, initiated in 2002, aimed to characterize clinical and laboratory data, whole body MRI detected lesions, and treatment responses in 37 juvenile patients with chronic non-bacterial osteomyelitis at a time when biological DMARDs were not yet standard therapy.
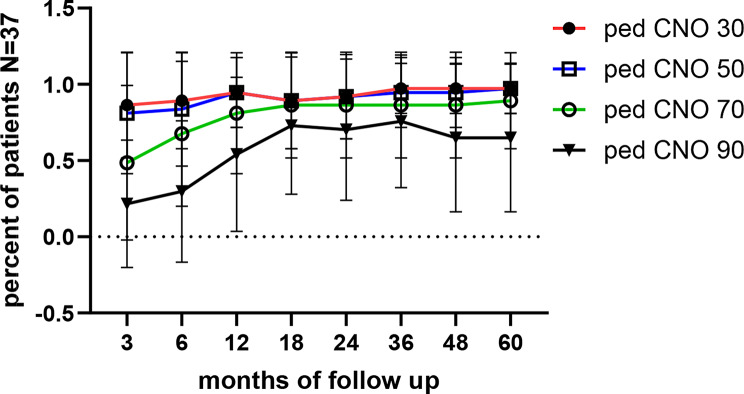
Methods: Patients were assessed at baseline and at 1 (without MRI), 3, 6, 12, 18, 24, 36, 48, 60 months. All patients received naproxen as first-line therapy. Clinical management allowed for escalation to sulfasalazine, pamidronate, and glucocorticoids as needed. Treatment response was evaluated using the pedCNO disease activity score (30/50/70/90% improvement). Further composite numeric disease activity (DA) scores- the CARRA CDAS and a new MRI DAS - were applied.
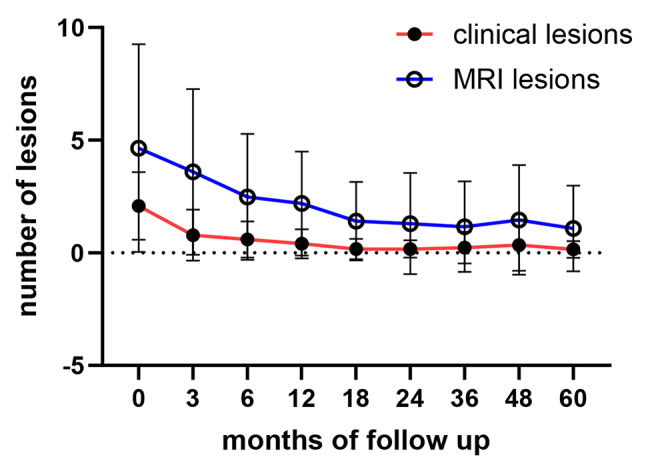
Results: The mean age at disease onset was 10.8 years, with a diagnostic delay of 5.8 months. Naproxen was the initial treatment in all patients. Second-line therapy was initiated in 10 patients due to inadequate improvement in physician global assessment of disease activity, patient-reported overall wellbeing or MRI lesions. Escalated therapies included sulfasalazine (n = 10), bisphosphonates (n = 1), methotrexate (n = 1), and short- (< 4 wks) or long-term oral glucocorticoids (n = 5 and n = 3, respectively). The mean number of clinical lesions decreased from 2.1 to 0.4 at 12 months and reached 0.15 at 60 months. MRI-detected lesions declined from 5.0 to 2.25 at 12 months and to 1.1 at 60 months.
Conclusion: Most children experienced favourable long-term outcomes. Clinical improvement occurred more rapidly than radiologic resolution. Patients with insufficient response to NSAIDs should be considered for a treat-to-target approach, including the use of conventional and biologic DMARDs.
Trial registration: A trial registration EUDRA CT was not available at the time the study was started. Informed consent was given by all parents.
期刊介绍:
Pediatric Rheumatology is an open access, peer-reviewed, online journal encompassing all aspects of clinical and basic research related to pediatric rheumatology and allied subjects.
The journal’s scope of diseases and syndromes include musculoskeletal pain syndromes, rheumatic fever and post-streptococcal syndromes, juvenile idiopathic arthritis, systemic lupus erythematosus, juvenile dermatomyositis, local and systemic scleroderma, Kawasaki disease, Henoch-Schonlein purpura and other vasculitides, sarcoidosis, inherited musculoskeletal syndromes, autoinflammatory syndromes, and others.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


