{"title":"Risk of anterior interosseous nerve injury during forearm surgery: a cadaveric study.","authors":"Arnaud Walch, Hugo Despert, Clément Jubelin, Laurent Mathieu, Camille Brenac, Thibault Druel","doi":"10.1007/s00068-025-02869-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The anterior interosseous nerve (AIN) is susceptible to injury during forearm surgery, particularly open reduction and internal fixation (ORIF) of radius fractures. This study aimed to analyze the anatomical relationships between the AIN and the radius to identify regions most vulnerable to iatrogenic injury.</p><p><strong>Methods: </strong>A cadaveric study was conducted on ten fresh, non-embalmed forearms. Standardized dissections were performed to assess the course of the AIN, its motor branches, and their proximity to bony landmarks. Measurements were taken using a graduated ruler, with reference to the radius, the bi-epicondylar and bi-styloid lines.</p><p><strong>Results: </strong>The AIN originated, on average, 13 mm from the radius, initially separated from the bone by the flexor digitorum profundus and flexor pollicis longus. The first branch to the flexor pollicis longus emerged at an average of 8 mm from the radius, marking the start of the nerve's close contact with the bone. The highest risk zone for AIN injury was identified at the junction of the proximal and middle thirds of the forearm.</p><p><strong>Conclusion: </strong>The AIN and its motor branches exhibit significant anatomical variability but consistently demonstrate proximity to the radius at the proximal-middle third junction. To minimize iatrogenic injury, care should be taken when exposing the anterior radius, particularly by avoiding excessive traction or deep retractor placement in this region.</p>","PeriodicalId":12064,"journal":{"name":"European Journal of Trauma and Emergency Surgery","volume":"51 1","pages":"197"},"PeriodicalIF":2.2000,"publicationDate":"2025-05-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12055948/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Trauma and Emergency Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00068-025-02869-9","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: The anterior interosseous nerve (AIN) is susceptible to injury during forearm surgery, particularly open reduction and internal fixation (ORIF) of radius fractures. This study aimed to analyze the anatomical relationships between the AIN and the radius to identify regions most vulnerable to iatrogenic injury.
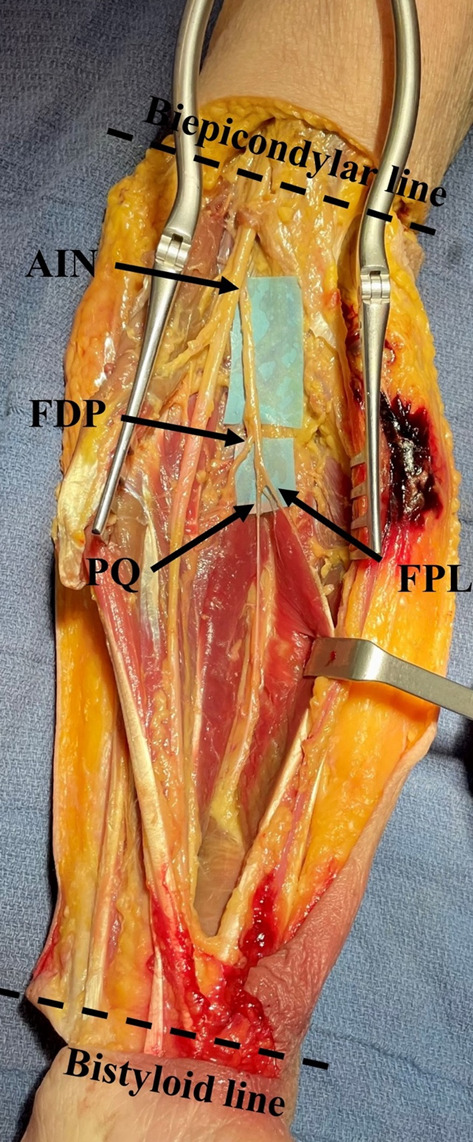
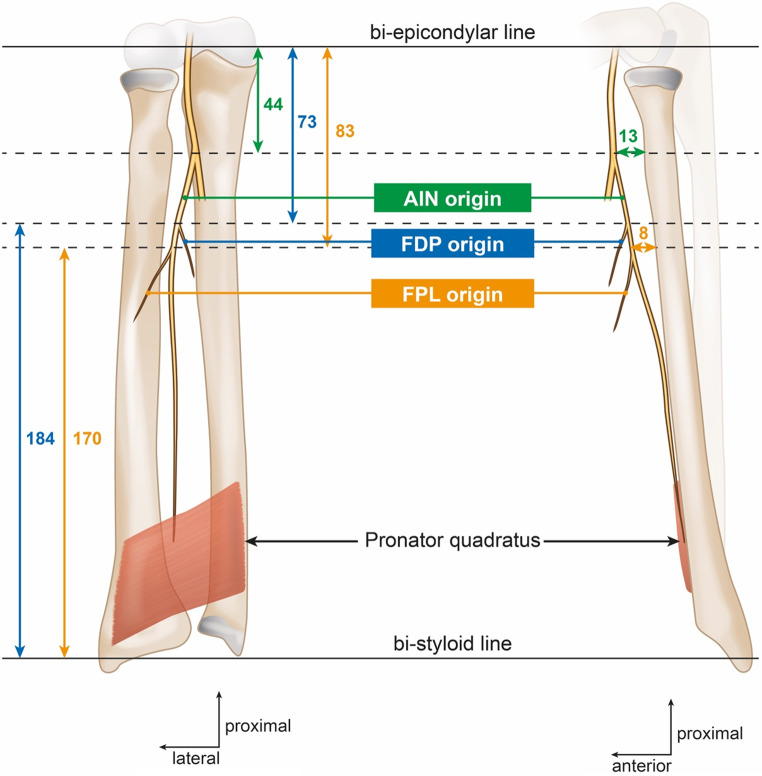
Methods: A cadaveric study was conducted on ten fresh, non-embalmed forearms. Standardized dissections were performed to assess the course of the AIN, its motor branches, and their proximity to bony landmarks. Measurements were taken using a graduated ruler, with reference to the radius, the bi-epicondylar and bi-styloid lines.
Results: The AIN originated, on average, 13 mm from the radius, initially separated from the bone by the flexor digitorum profundus and flexor pollicis longus. The first branch to the flexor pollicis longus emerged at an average of 8 mm from the radius, marking the start of the nerve's close contact with the bone. The highest risk zone for AIN injury was identified at the junction of the proximal and middle thirds of the forearm.
Conclusion: The AIN and its motor branches exhibit significant anatomical variability but consistently demonstrate proximity to the radius at the proximal-middle third junction. To minimize iatrogenic injury, care should be taken when exposing the anterior radius, particularly by avoiding excessive traction or deep retractor placement in this region.
期刊介绍:
The European Journal of Trauma and Emergency Surgery aims to open an interdisciplinary forum that allows for the scientific exchange between basic and clinical science related to pathophysiology, diagnostics and treatment of traumatized patients. The journal covers all aspects of clinical management, operative treatment and related research of traumatic injuries.
Clinical and experimental papers on issues relevant for the improvement of trauma care are published. Reviews, original articles, short communications and letters allow the appropriate presentation of major and minor topics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


