Short-term outcomes of periacetabular osteotomy versus periacetabular osteotomy with concomitant femoral osteochondroplasty: a propensity matched analysis.
Nathan V Houlihan, Daniel J Sucato, Tanner Thornton, Jeffrey J Nepple, John C Clohisy, Wudbhav N Sankar
{"title":"Short-term outcomes of periacetabular osteotomy versus periacetabular osteotomy with concomitant femoral osteochondroplasty: a propensity matched analysis.","authors":"Nathan V Houlihan, Daniel J Sucato, Tanner Thornton, Jeffrey J Nepple, John C Clohisy, Wudbhav N Sankar","doi":"10.1093/jhps/hnae046","DOIUrl":null,"url":null,"abstract":"<p><p>This study compared outcomes of periacetabular osteotomy (PAO) with and without femoral osteochondroplasty (OCP) in treating symptomatic acetabular dysplasia through propensity score matching. Data from a prospective multicenter cohort of patients undergoing PAO from 2007 to 2014 were analyzed. Inclusion criteria were a lateral center edge angle <25°. The exclusion criteria were history of previous procedure and age >45 years. A 2- to 5-year follow-up interval was utilized; patients outside this follow-up window were excluded. Propensity matching variables included sex, baseline hip internal rotation at 90° flexion, preoperative alpha angle, lateral center edge angle, modified Harris Hip score (mHHS), and arthroscopy at the time of surgery. Propensity scores were calculated using logistic regression with treatment as the dependent variable. Clinical failure was defined as failure to meet the minimal clinically important difference and patient acceptable symptom state for mHHS or a need for reoperation. There were 219 patients that met the inclusion criteria. Of these, 116 patients were matched, representing 58 pairs (PAO/OCP = 58; PAO without OCP = 58). Preoperative functional scores were similar between groups. At mean 4.1 years follow-up, there were no significant differences in the rates of clinical failure or reoperation between the two groups [PAO/OCP = 13 (22%), PAO without OCP = 8 (14%); <i>P</i> = .23] Similarly, the final mHHS was 83.2 ± 16.2 for the PAO/OCP group and 84.1 ± 15.9 for the isolated PAO group, with no significant difference (<i>P</i> = .74). In the treatment of symptomatic acetabular dysplasia, isolated PAO is noninferior to combined PAO/OCP at short-term follow-up in patients who are likely to be treated by either method.</p>","PeriodicalId":48583,"journal":{"name":"Journal of Hip Preservation Surgery","volume":"12 1","pages":"40-45"},"PeriodicalIF":1.1000,"publicationDate":"2024-12-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12051856/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Hip Preservation Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/jhps/hnae046","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
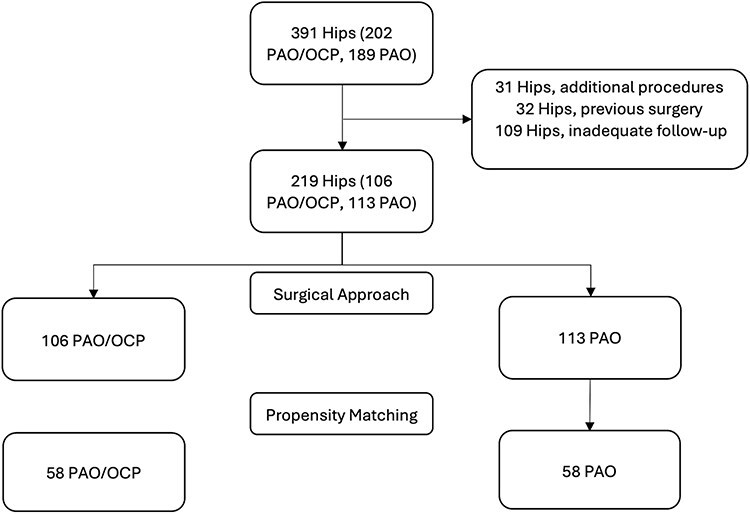
This study compared outcomes of periacetabular osteotomy (PAO) with and without femoral osteochondroplasty (OCP) in treating symptomatic acetabular dysplasia through propensity score matching. Data from a prospective multicenter cohort of patients undergoing PAO from 2007 to 2014 were analyzed. Inclusion criteria were a lateral center edge angle <25°. The exclusion criteria were history of previous procedure and age >45 years. A 2- to 5-year follow-up interval was utilized; patients outside this follow-up window were excluded. Propensity matching variables included sex, baseline hip internal rotation at 90° flexion, preoperative alpha angle, lateral center edge angle, modified Harris Hip score (mHHS), and arthroscopy at the time of surgery. Propensity scores were calculated using logistic regression with treatment as the dependent variable. Clinical failure was defined as failure to meet the minimal clinically important difference and patient acceptable symptom state for mHHS or a need for reoperation. There were 219 patients that met the inclusion criteria. Of these, 116 patients were matched, representing 58 pairs (PAO/OCP = 58; PAO without OCP = 58). Preoperative functional scores were similar between groups. At mean 4.1 years follow-up, there were no significant differences in the rates of clinical failure or reoperation between the two groups [PAO/OCP = 13 (22%), PAO without OCP = 8 (14%); P = .23] Similarly, the final mHHS was 83.2 ± 16.2 for the PAO/OCP group and 84.1 ± 15.9 for the isolated PAO group, with no significant difference (P = .74). In the treatment of symptomatic acetabular dysplasia, isolated PAO is noninferior to combined PAO/OCP at short-term follow-up in patients who are likely to be treated by either method.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


