{"title":"Life-threatening interstitial lung disease with adjuvant osimertinib after complete resection of non-small cell lung cancer: a case report.","authors":"Takatoshi Osako, Teruhisa Takuwa, Yusuke Shindo","doi":"10.21037/acr-24-203","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This case report describes a rare and severe instance of osimertinib-induced interstitial lung disease (ILD) requiring intubation and mechanical ventilation during postoperative adjuvant therapy following lung cancer resection. This is the most severe reported case, necessitating intensive care. While severe ILD during adjuvant therapy is uncommon, its incidence may increase as osimertinib use expands.</p><p><strong>Case description: </strong>A 68-year-old nonsmoking female with no history of ILD underwent left lower lobectomy for epidermal growth factor receptor (EGFR)-mutated non-small cell lung cancer (stage IIB, pT3N0M0). Following adjuvant cisplatin and vinorelbine chemotherapy, osimertinib (80 mg/day) was initiated. Thirty-five days later, she developed acute respiratory distress and hypoxemia [saturation of percutaneous oxygen (SpO2) 78% on room air], rendering her unable to walk without assistance. Chest computed tomography (CT) revealed diffuse ground-glass opacities across both lungs. Osimertinib was discontinued, and methylprednisolone (500 mg/day) was started; however, oxygenation rapidly deteriorated, leading to intubation and mechanical ventilation the following day. The patient was diagnosed with severe grade IV ILD induced by osimertinib. After 5 days of methylprednisolone, treatment was switched to prednisolone (60 mg/day), but oxygenation worsened, and pulmonary infiltrates reappeared on CT. Methylprednisolone (500 mg/day) was reintroduced for 5 days. The partial pressure of oxygen in the arterial blood (PaO2)/fraction of inspired oxygen (FiO2) ratio then improved, and prednisolone was gradually tapered from 1 mg/kg with a weekly reduction of 10 mg based on clinical and radiologic improvement. The patient was discharged on day 72 with prednisolone 30 mg/day. Although respiratory symptoms improved significantly, she required long-term home oxygen therapy due to residual hypoxemia during exertion.</p><p><strong>Conclusions: </strong>This case underscores the potentially life-threatening nature of osimertinib-induced ILD in adjuvant therapy. Careful patient selection, thorough risk assessment, and vigilant monitoring are crucial for early detection and management. Given the increasing use of osimertinib in postoperative settings, further research is needed to better understand and mitigate the risks associated with this therapy.</p>","PeriodicalId":29752,"journal":{"name":"AME Case Reports","volume":"9 ","pages":"56"},"PeriodicalIF":0.7000,"publicationDate":"2025-04-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12053883/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AME Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/acr-24-203","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: This case report describes a rare and severe instance of osimertinib-induced interstitial lung disease (ILD) requiring intubation and mechanical ventilation during postoperative adjuvant therapy following lung cancer resection. This is the most severe reported case, necessitating intensive care. While severe ILD during adjuvant therapy is uncommon, its incidence may increase as osimertinib use expands.
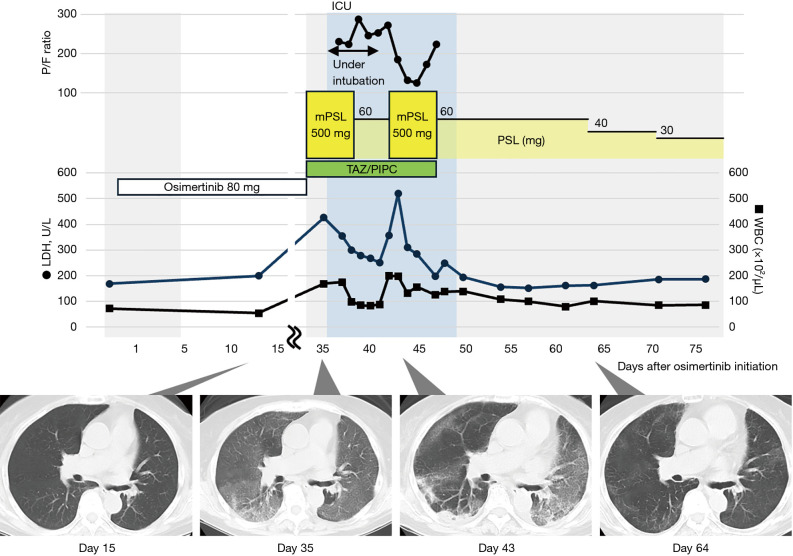
Case description: A 68-year-old nonsmoking female with no history of ILD underwent left lower lobectomy for epidermal growth factor receptor (EGFR)-mutated non-small cell lung cancer (stage IIB, pT3N0M0). Following adjuvant cisplatin and vinorelbine chemotherapy, osimertinib (80 mg/day) was initiated. Thirty-five days later, she developed acute respiratory distress and hypoxemia [saturation of percutaneous oxygen (SpO2) 78% on room air], rendering her unable to walk without assistance. Chest computed tomography (CT) revealed diffuse ground-glass opacities across both lungs. Osimertinib was discontinued, and methylprednisolone (500 mg/day) was started; however, oxygenation rapidly deteriorated, leading to intubation and mechanical ventilation the following day. The patient was diagnosed with severe grade IV ILD induced by osimertinib. After 5 days of methylprednisolone, treatment was switched to prednisolone (60 mg/day), but oxygenation worsened, and pulmonary infiltrates reappeared on CT. Methylprednisolone (500 mg/day) was reintroduced for 5 days. The partial pressure of oxygen in the arterial blood (PaO2)/fraction of inspired oxygen (FiO2) ratio then improved, and prednisolone was gradually tapered from 1 mg/kg with a weekly reduction of 10 mg based on clinical and radiologic improvement. The patient was discharged on day 72 with prednisolone 30 mg/day. Although respiratory symptoms improved significantly, she required long-term home oxygen therapy due to residual hypoxemia during exertion.
Conclusions: This case underscores the potentially life-threatening nature of osimertinib-induced ILD in adjuvant therapy. Careful patient selection, thorough risk assessment, and vigilant monitoring are crucial for early detection and management. Given the increasing use of osimertinib in postoperative settings, further research is needed to better understand and mitigate the risks associated with this therapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


