Ai-Hui Li, Yang Li, Meng-Shi Li, Zhuo-Ran Song, Ji-Cheng Lv, Hong Zhang, Xiao-Juan Yu, Xu-Jie Zhou
{"title":"Repeated Kidney Biopsy in Membranoproliferative Glomerulonephritis.","authors":"Ai-Hui Li, Yang Li, Meng-Shi Li, Zhuo-Ran Song, Ji-Cheng Lv, Hong Zhang, Xiao-Juan Yu, Xu-Jie Zhou","doi":"10.1159/000545727","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Membranoproliferative glomerulonephritis (MPGN) is a heterogeneous pattern of glomerular injury. Repeated kidney biopsies may elucidate pathogenic mechanisms and guide diagnostic strategies.</p><p><strong>Methods: </strong>We included 82 patients diagnosed with MPGN by kidney biopsy who underwent at least two biopsies between 1997 and 2023 at Peking University First Hospital. Clinical and pathological data were analyzed retrospectively.</p><p><strong>Results: </strong>Of 342 MPGN patients, 95 (28%) had repeated biopsies (0.9-4.0 years apart). This incidence was higher than in other glomerulonephropathies under immunosuppression. Among the 82 patients analyzed (excluding kidney transplants and ≤3-month biopsy intervals), 42 were initially diagnosed with non-MPGN pathology. At the second biopsy, proteinuria increased (from 2.9 to 6.3 g/day), eGFR declined (from 76 to 47 mL/min/1.73 m<sup>2</sup>), and renal C3 deposition was stronger (<i>p</i> = 0.04). Thirty patients (37%) had etiological reclassification, mostly to monoclonal gammopathy of renal significance (MGRS). Compared to idiopathic MPGN, MGRS patients were older (53 vs. 35 years) and had worse renal function (eGFR 57 vs. 81 mL/min/1.73 m<sup>2</sup>) but slower eGFR decline (-7 vs. -12 mL/min/1.73 m<sup>2</sup>/year). Most MGRS patients (64%) remained negative for monoclonal protein in serum or urine immunofixation, necessitating repeat biopsy and clone-directed therapy.</p><p><strong>Conclusion: </strong>In this study, about half and one-third of patients underwent morphological and etiological reclassification, respectively. Stronger complement deposition may drive morphological changes. Repeated kidney biopsies are crucial for diagnosing MGRS, especially in patients with negative immunofixation.</p>","PeriodicalId":17830,"journal":{"name":"Kidney Diseases","volume":"11 1","pages":"258-269"},"PeriodicalIF":3.1000,"publicationDate":"2025-04-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12058111/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Kidney Diseases","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000545727","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Membranoproliferative glomerulonephritis (MPGN) is a heterogeneous pattern of glomerular injury. Repeated kidney biopsies may elucidate pathogenic mechanisms and guide diagnostic strategies.
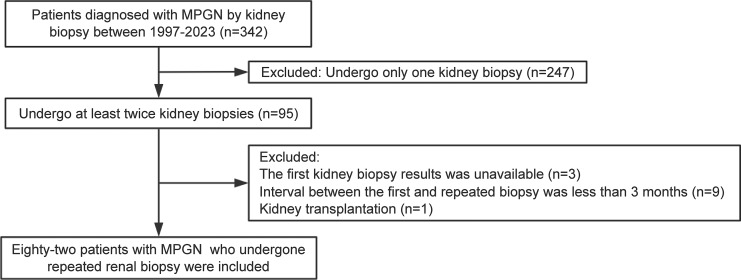
Methods: We included 82 patients diagnosed with MPGN by kidney biopsy who underwent at least two biopsies between 1997 and 2023 at Peking University First Hospital. Clinical and pathological data were analyzed retrospectively.
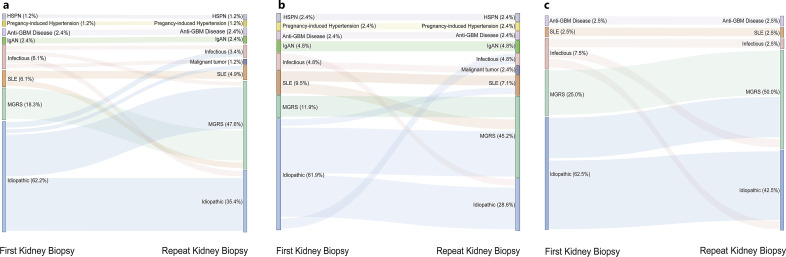
Results: Of 342 MPGN patients, 95 (28%) had repeated biopsies (0.9-4.0 years apart). This incidence was higher than in other glomerulonephropathies under immunosuppression. Among the 82 patients analyzed (excluding kidney transplants and ≤3-month biopsy intervals), 42 were initially diagnosed with non-MPGN pathology. At the second biopsy, proteinuria increased (from 2.9 to 6.3 g/day), eGFR declined (from 76 to 47 mL/min/1.73 m2), and renal C3 deposition was stronger (p = 0.04). Thirty patients (37%) had etiological reclassification, mostly to monoclonal gammopathy of renal significance (MGRS). Compared to idiopathic MPGN, MGRS patients were older (53 vs. 35 years) and had worse renal function (eGFR 57 vs. 81 mL/min/1.73 m2) but slower eGFR decline (-7 vs. -12 mL/min/1.73 m2/year). Most MGRS patients (64%) remained negative for monoclonal protein in serum or urine immunofixation, necessitating repeat biopsy and clone-directed therapy.
Conclusion: In this study, about half and one-third of patients underwent morphological and etiological reclassification, respectively. Stronger complement deposition may drive morphological changes. Repeated kidney biopsies are crucial for diagnosing MGRS, especially in patients with negative immunofixation.
期刊介绍:
''Kidney Diseases'' aims to provide a platform for Asian and Western research to further and support communication and exchange of knowledge. Review articles cover the most recent clinical and basic science relevant to the entire field of nephrological disorders, including glomerular diseases, acute and chronic kidney injury, tubulo-interstitial disease, hypertension and metabolism-related disorders, end-stage renal disease, and genetic kidney disease. Special articles are prepared by two authors, one from East and one from West, which compare genetics, epidemiology, diagnosis methods, and treatment options of a disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


