Vimal Desai, Priscilla H Chan, Kathryn E Royse, Ronald A Navarro, Glenn R Diekmann, Kent T Yamaguchi, Elizabeth W Paxton, Chunyuan Qiu
{"title":"Factors Associated with Mortality and Short-Term Patient Outcomes for Hip Fracture Repair in the Elderly Based on Preoperative Anticoagulation Status.","authors":"Vimal Desai, Priscilla H Chan, Kathryn E Royse, Ronald A Navarro, Glenn R Diekmann, Kent T Yamaguchi, Elizabeth W Paxton, Chunyuan Qiu","doi":"10.3390/geriatrics10020054","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> The one-year mortality risk for elderly patients undergoing proximal femur fracture repair surgery is three to four times higher compared to the general population. Other than time to surgery, risk factors for postoperative morbidity and mortality following surgery are poorly understood in the elderly. We sought to identify risk factors associated with morbidity and mortality in geriatric patients by anticoagulation status undergoing hip fracture repair. <b>Methods:</b> Patients aged ≥65 years undergoing surgery for hip fracture repair were included (2009-2019) from a US-based hip fracture registry. Factors associated with 90-day mortality were determined using multivariable logistic regression and stratified by antithrombotic agent medication use prior to surgery. Direct oral anticoagulation (DOAC) medications were the largest group, and all antithrombotic agents were included in the delineation. <b>Results:</b> A total of 35,463 patients were identified, and 87.1% (<i>N</i> = 30,902) were DOAC-naïve. Risk factors for 90-day mortality in DOAC-naïve patients were an American Society of Anesthesiologist's (ASA) classification ≥3 (odds ratio [OR] = 2.56, 95% confidence interval [CI] = 2.24-2.93), preoperative myocardial infarction (OR = 1.87, 95% CI = 1.33-2.64), male gender (OR = 1.73, 95% CI = 1.59-1.88), congestive heart failure (CHF) (OR = 1.64, 95% CI = 1.50-1.80), psychoses (OR = 1.27, 95% CI = 1.15-1.42), renal failure (OR = 1.29, 95% CI = 1.19-1.40), smoking history (OR = 1.19, 95% CI = 1.09-1.29), chronic pulmonary disease (OR = 1.14, 95% CI = 1.05-1.25), increasing age (OR = 1.07, 95% CI = 1.06-1.07), and decreasing body mass index (BMI) (OR = 1.06, 95% CI = 1.05-1.08). Identified factors for mortality in the DOAC group also included ASA classification ≥3 (OR = 2.15, 95% CI = 1.44-3.20), male gender (OR = 1.68, 95% CI = 1.41-2.01), CHF (OR = 1.45, 95% CI = 1.22-1.73), chronic pulmonary disease (OR = 1.34, 95% CI = 1.12-1.61), decreasing BMI (OR = 1.04, 95% CI = 1.02-1.06), and increasing age (OR = 1.02, 95% CI = 1.01-1.03). <b>Conclusions:</b> Regardless of preoperative DOAC status, ASA classification, gender, CHF, chronic pulmonary disease, lower BMI, and higher age are associated with an increased risk of mortality. Some of these comorbidities can be utilized for risk stratification prior to surgery.</p>","PeriodicalId":12653,"journal":{"name":"Geriatrics","volume":"10 2","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2025-04-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12026724/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Geriatrics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/geriatrics10020054","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
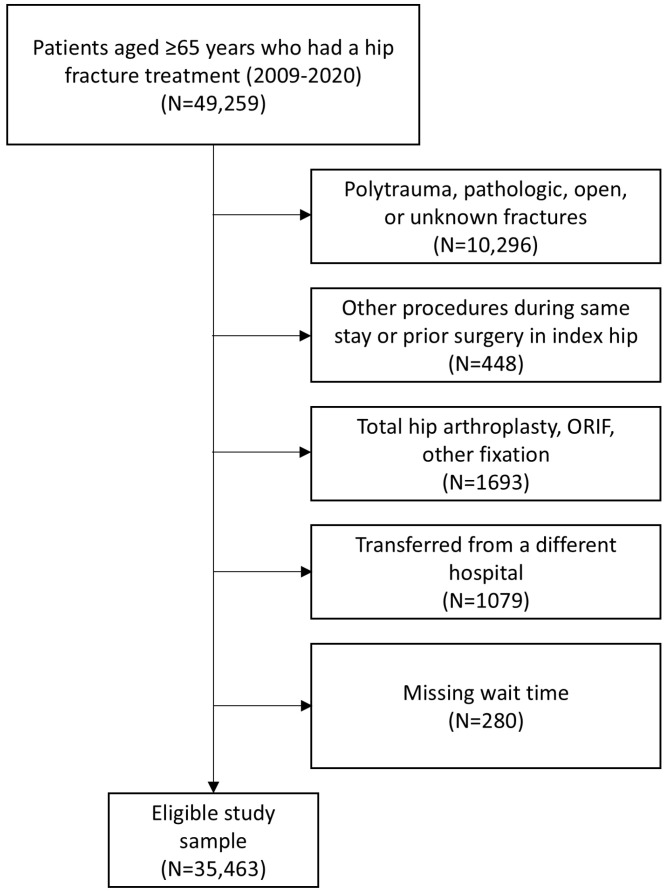
Background: The one-year mortality risk for elderly patients undergoing proximal femur fracture repair surgery is three to four times higher compared to the general population. Other than time to surgery, risk factors for postoperative morbidity and mortality following surgery are poorly understood in the elderly. We sought to identify risk factors associated with morbidity and mortality in geriatric patients by anticoagulation status undergoing hip fracture repair. Methods: Patients aged ≥65 years undergoing surgery for hip fracture repair were included (2009-2019) from a US-based hip fracture registry. Factors associated with 90-day mortality were determined using multivariable logistic regression and stratified by antithrombotic agent medication use prior to surgery. Direct oral anticoagulation (DOAC) medications were the largest group, and all antithrombotic agents were included in the delineation. Results: A total of 35,463 patients were identified, and 87.1% (N = 30,902) were DOAC-naïve. Risk factors for 90-day mortality in DOAC-naïve patients were an American Society of Anesthesiologist's (ASA) classification ≥3 (odds ratio [OR] = 2.56, 95% confidence interval [CI] = 2.24-2.93), preoperative myocardial infarction (OR = 1.87, 95% CI = 1.33-2.64), male gender (OR = 1.73, 95% CI = 1.59-1.88), congestive heart failure (CHF) (OR = 1.64, 95% CI = 1.50-1.80), psychoses (OR = 1.27, 95% CI = 1.15-1.42), renal failure (OR = 1.29, 95% CI = 1.19-1.40), smoking history (OR = 1.19, 95% CI = 1.09-1.29), chronic pulmonary disease (OR = 1.14, 95% CI = 1.05-1.25), increasing age (OR = 1.07, 95% CI = 1.06-1.07), and decreasing body mass index (BMI) (OR = 1.06, 95% CI = 1.05-1.08). Identified factors for mortality in the DOAC group also included ASA classification ≥3 (OR = 2.15, 95% CI = 1.44-3.20), male gender (OR = 1.68, 95% CI = 1.41-2.01), CHF (OR = 1.45, 95% CI = 1.22-1.73), chronic pulmonary disease (OR = 1.34, 95% CI = 1.12-1.61), decreasing BMI (OR = 1.04, 95% CI = 1.02-1.06), and increasing age (OR = 1.02, 95% CI = 1.01-1.03). Conclusions: Regardless of preoperative DOAC status, ASA classification, gender, CHF, chronic pulmonary disease, lower BMI, and higher age are associated with an increased risk of mortality. Some of these comorbidities can be utilized for risk stratification prior to surgery.
期刊介绍:
• Geriatric biology
• Geriatric health services research
• Geriatric medicine research
• Geriatric neurology, stroke, cognition and oncology
• Geriatric surgery
• Geriatric physical functioning, physical health and activity
• Geriatric psychiatry and psychology
• Geriatric nutrition
• Geriatric epidemiology
• Geriatric rehabilitation

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


