Comparison of Outcomes After Revascularization for Acute Lower Limb Ischemia in Patients with and without Type 2 Diabetes Mellitus - A Nationwide Registry Study.
Emil Karonen, Frida Eek, Isabel Drake, Talha Butt, Hanne Krage Carlsen, Björn Eliasson, Anders Gottsäter, Stefan Acosta
{"title":"Comparison of Outcomes After Revascularization for Acute Lower Limb Ischemia in Patients with and without Type 2 Diabetes Mellitus - A Nationwide Registry Study.","authors":"Emil Karonen, Frida Eek, Isabel Drake, Talha Butt, Hanne Krage Carlsen, Björn Eliasson, Anders Gottsäter, Stefan Acosta","doi":"10.2147/VHRM.S497866","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Acute lower limb ischemia (ALI) is a life and limb threatening event often affecting patients with type 2 diabetes mellitus (T2DM). Little is known about how T2DM affects the risk of adverse events in patients revascularized for ALI. This study aimed to investigate if there were differences in major outcomes between ALI patients with and without T2DM.</p><p><strong>Methods: </strong>Between 2010 and 2014, 615 patients underwent revascularization for ALI, according to the Swedish Vascular Registry (SWEDVASC). Using the National Diabetes Registry (NDR), 245 (39.8%) of the patients were identified as having T2DM. Uni- and multivariable Cox or logistic regression analyses were performed to evaluate risk differences for major amputation, mortality, major adverse cardiovascular events (MACE), and fasciotomy between patients with and without T2DM.</p><p><strong>Results: </strong>The rates of major amputation and mortality at one year were 32.7% and 21.6% in the T2DM group, compared to 21.9% and 31.9% in the non-DM group, respectively, resulting in a hazard ratio (HR) of 1.52 (95% confidence interval [CI] 1.12-2.07) for major amputation and HR of 0.64 (95% CI 0.46-0.88) for mortality. At one year, the HR for major amputation was 1.45 (95% CI 0.99-2.11), HR for mortality 0.92 (95% CI 0.61-1.39), HR for combined major amputation/mortality 1.27 (95% CI 0.94-1.72), and HR for MACE 1.24 (95% CI 0.92-1.67) for those with T2DM compared to those without in the multivariable Cox-regression analyses. The multivariable logistic regression analysis showed significantly lower odds of fasciotomy, OR 0.1 (95% CI 0.01-0.51) in the T2DM-group.</p><p><strong>Conclusion: </strong>T2DM was not significantly associated with higher hazard of major amputation, mortality, combined major amputation/mortality, or MACE after revascularization for ALI, compared to patients without T2DM. Patients with T2DM had significantly lower odds of fasciotomy.</p>","PeriodicalId":23597,"journal":{"name":"Vascular Health and Risk Management","volume":"21 ","pages":"229-238"},"PeriodicalIF":2.8000,"publicationDate":"2025-04-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11998955/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Vascular Health and Risk Management","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/VHRM.S497866","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Acute lower limb ischemia (ALI) is a life and limb threatening event often affecting patients with type 2 diabetes mellitus (T2DM). Little is known about how T2DM affects the risk of adverse events in patients revascularized for ALI. This study aimed to investigate if there were differences in major outcomes between ALI patients with and without T2DM.
Methods: Between 2010 and 2014, 615 patients underwent revascularization for ALI, according to the Swedish Vascular Registry (SWEDVASC). Using the National Diabetes Registry (NDR), 245 (39.8%) of the patients were identified as having T2DM. Uni- and multivariable Cox or logistic regression analyses were performed to evaluate risk differences for major amputation, mortality, major adverse cardiovascular events (MACE), and fasciotomy between patients with and without T2DM.
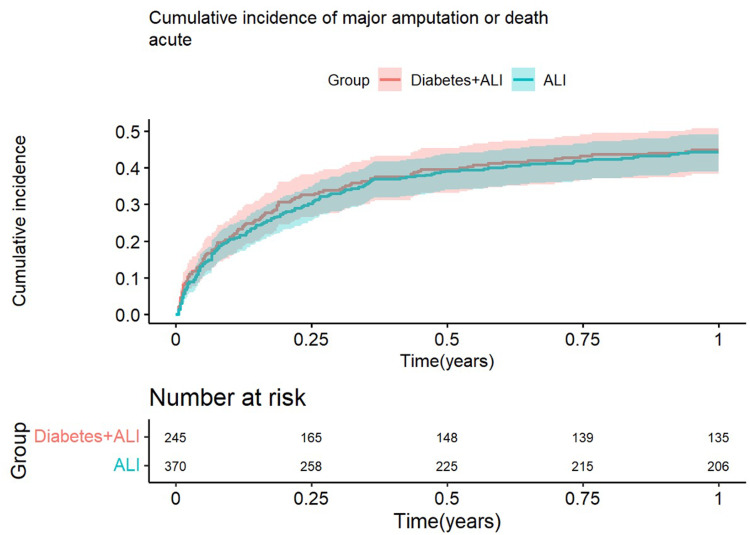
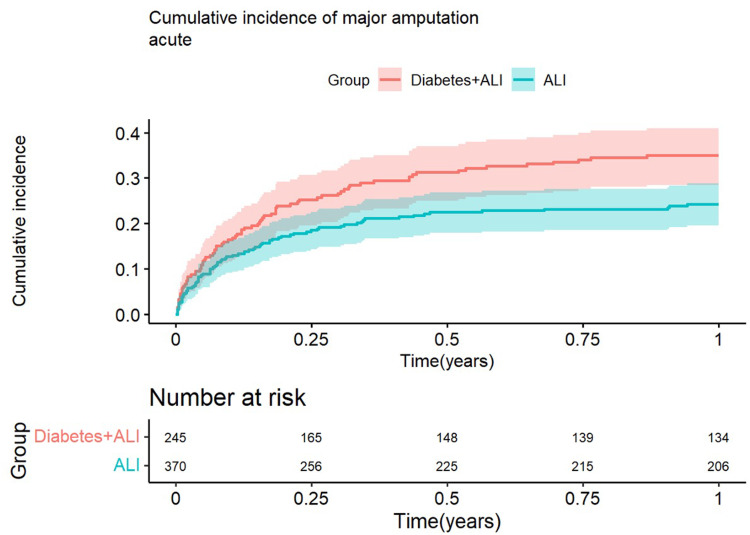
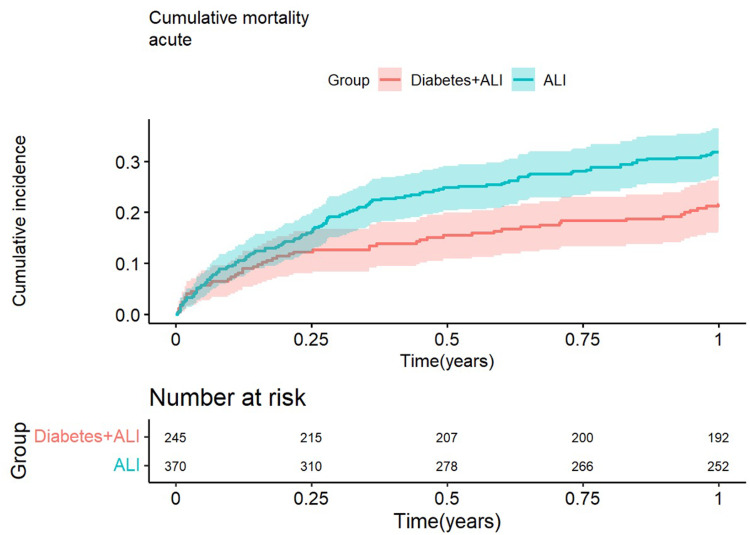
Results: The rates of major amputation and mortality at one year were 32.7% and 21.6% in the T2DM group, compared to 21.9% and 31.9% in the non-DM group, respectively, resulting in a hazard ratio (HR) of 1.52 (95% confidence interval [CI] 1.12-2.07) for major amputation and HR of 0.64 (95% CI 0.46-0.88) for mortality. At one year, the HR for major amputation was 1.45 (95% CI 0.99-2.11), HR for mortality 0.92 (95% CI 0.61-1.39), HR for combined major amputation/mortality 1.27 (95% CI 0.94-1.72), and HR for MACE 1.24 (95% CI 0.92-1.67) for those with T2DM compared to those without in the multivariable Cox-regression analyses. The multivariable logistic regression analysis showed significantly lower odds of fasciotomy, OR 0.1 (95% CI 0.01-0.51) in the T2DM-group.
Conclusion: T2DM was not significantly associated with higher hazard of major amputation, mortality, combined major amputation/mortality, or MACE after revascularization for ALI, compared to patients without T2DM. Patients with T2DM had significantly lower odds of fasciotomy.
急性下肢缺血(Acute lower limb ischemia, ALI)是2型糖尿病(T2DM)患者常发生的危及生命和肢体的事件。对于T2DM如何影响ALI患者血运重建术中不良事件的风险知之甚少。本研究旨在探讨ALI患者合并和不合并T2DM的主要结局是否存在差异。方法:根据瑞典血管登记处(SWEDVASC)的数据,2010年至2014年间,615例ALI患者接受了血运重建术。使用国家糖尿病登记处(NDR), 245例(39.8%)患者被确定为T2DM。采用单变量和多变量Cox或logistic回归分析来评估T2DM患者和非T2DM患者主要截肢、死亡率、主要不良心血管事件(MACE)和筋膜切开术的风险差异。结果:T2DM组1年主要截肢率和死亡率分别为32.7%和21.6%,非dm组分别为21.9%和31.9%,导致主要截肢的风险比(HR)为1.52(95%可信区间[CI] 1.12-2.07),死亡率的风险比(HR)为0.64(95%可信区间[CI] 0.46-0.88)。在多变量cox回归分析中,1年时,T2DM患者与非T2DM患者相比,主要截肢的HR为1.45 (95% CI 0.99-2.11),死亡率HR为0.92 (95% CI 0.61-1.39),合并主要截肢/死亡率HR为1.27 (95% CI 0.94-1.72), MACE HR为1.24 (95% CI 0.92-1.67)。多变量logistic回归分析显示,t2dm组筋膜切开术的几率显著降低,OR为0.1 (95% CI 0.01-0.51)。结论:与非T2DM患者相比,T2DM与ALI大截肢、死亡率、合并大截肢/死亡率或血管重建术后MACE的高风险无显著相关。T2DM患者行筋膜切开术的几率明显较低。
期刊介绍:
An international, peer-reviewed journal of therapeutics and risk management, focusing on concise rapid reporting of clinical studies on the processes involved in the maintenance of vascular health; the monitoring, prevention, and treatment of vascular disease and its sequelae; and the involvement of metabolic disorders, particularly diabetes. In addition, the journal will also seek to define drug usage in terms of ultimate uptake and acceptance by the patient and healthcare professional.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


