Garrett Thomas Coleman, Rawan Dayah, Suimin Qiu, Gurinder Luthra
{"title":"Cap Polyposis Syndrome Imitating Inflammatory Bowel Disease with Polyps Extending to the Terminal Ileum.","authors":"Garrett Thomas Coleman, Rawan Dayah, Suimin Qiu, Gurinder Luthra","doi":"10.1159/000545182","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Cap polyposis syndrome is a rare subtype of mucosal prolapse disease characterized by erythematous, inflammatory colonic polyps covered by a cap of fibrinopurulent mucous. Although a benign condition, patients may present with significant symptoms that can be suggestive of inflammatory bowel disease or colorectal cancer.</p><p><strong>Case presentation: </strong>We describe the case of a 34-year-old male who presented with a 5-month history of diarrhea and 40-lb weight loss following hospitalization for enterotoxigenic <i>Escherichia coli</i> colitis. The patient had a past medical history significant for prior colonoscopy revealing hundreds of polyps and a father who died of colorectal cancer at age 45. Multiple repeat infectious stool workups were negative, and antibiotics failed to resolve the patient's symptoms. The patient underwent endoscopy which revealed numerous polyps from the rectum to the terminal ileum that appeared similarly to pseudopolyps giving concern for inflammatory bowel disease. Subsequent histology demonstrated surface erosion and inflammation without dysplasia. Review of endoscopy showed inflammatory polyps with a cap of fibrinopurulent mucous. In the absence of chronic inflammation (C-reactive protein was within normal limits following hospitalization), endoscopic and histologic findings were suggestive of cap polyposis syndrome.</p><p><strong>Conclusion: </strong>Cap polyposis is diagnosed endoscopically and histologically. While most cases of cap polyposis are confined to the distal colon and rectum, we believe that this is the first case of cap polyposis syndrome extending to the terminal ileum. Treatment of cap polyposis syndrome is dependent on the severity of symptoms.</p>","PeriodicalId":9614,"journal":{"name":"Case Reports in Gastroenterology","volume":"19 1","pages":"314-319"},"PeriodicalIF":0.6000,"publicationDate":"2025-05-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12052363/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000545182","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Cap polyposis syndrome is a rare subtype of mucosal prolapse disease characterized by erythematous, inflammatory colonic polyps covered by a cap of fibrinopurulent mucous. Although a benign condition, patients may present with significant symptoms that can be suggestive of inflammatory bowel disease or colorectal cancer.
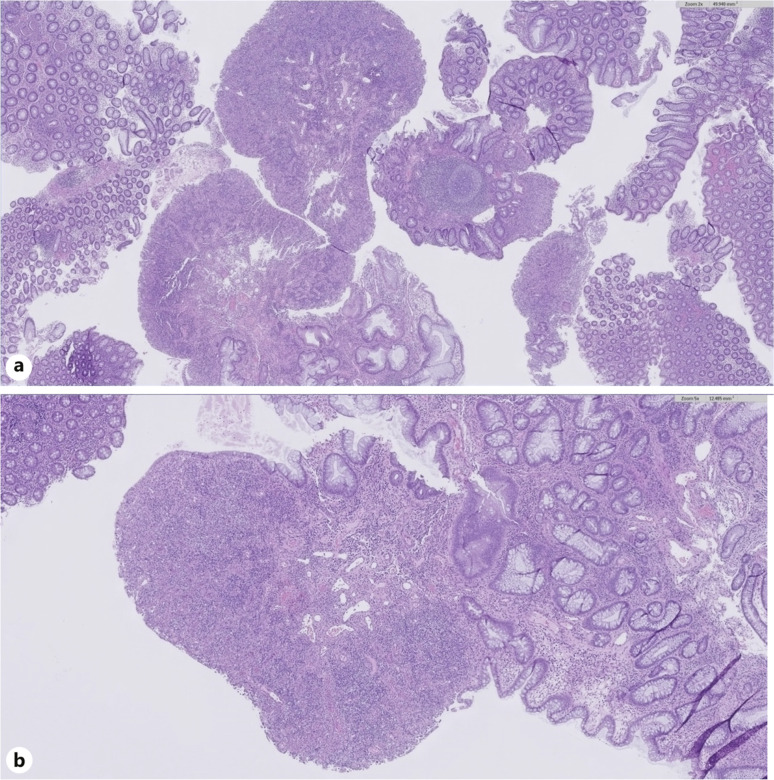
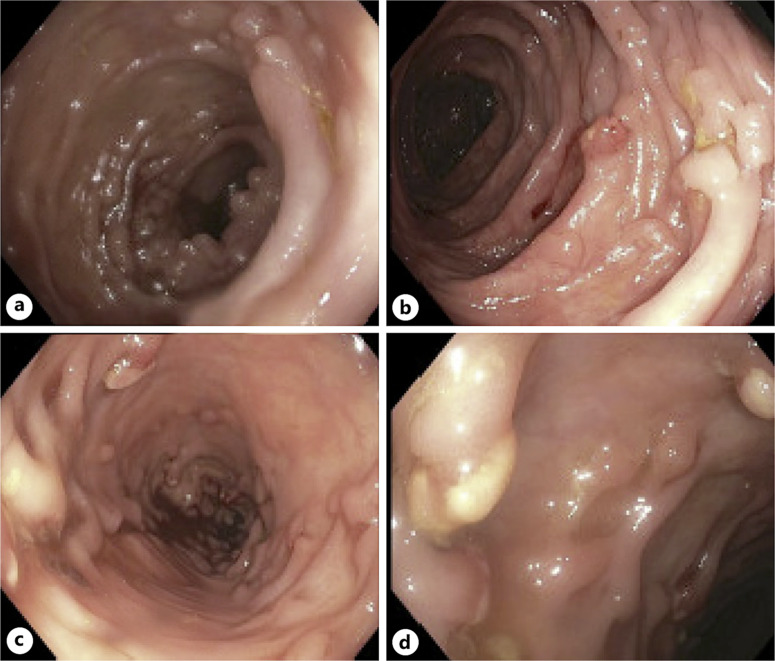
Case presentation: We describe the case of a 34-year-old male who presented with a 5-month history of diarrhea and 40-lb weight loss following hospitalization for enterotoxigenic Escherichia coli colitis. The patient had a past medical history significant for prior colonoscopy revealing hundreds of polyps and a father who died of colorectal cancer at age 45. Multiple repeat infectious stool workups were negative, and antibiotics failed to resolve the patient's symptoms. The patient underwent endoscopy which revealed numerous polyps from the rectum to the terminal ileum that appeared similarly to pseudopolyps giving concern for inflammatory bowel disease. Subsequent histology demonstrated surface erosion and inflammation without dysplasia. Review of endoscopy showed inflammatory polyps with a cap of fibrinopurulent mucous. In the absence of chronic inflammation (C-reactive protein was within normal limits following hospitalization), endoscopic and histologic findings were suggestive of cap polyposis syndrome.
Conclusion: Cap polyposis is diagnosed endoscopically and histologically. While most cases of cap polyposis are confined to the distal colon and rectum, we believe that this is the first case of cap polyposis syndrome extending to the terminal ileum. Treatment of cap polyposis syndrome is dependent on the severity of symptoms.
Cap polyposis综合征是一种罕见的粘膜脱垂病亚型,其特征是红斑性炎性结肠息肉被纤维蛋白脓性粘膜覆盖。虽然是一种良性疾病,但患者可能会出现提示炎症性肠病或结直肠癌的显著症状。病例介绍:我们报告一例34岁男性,因产肠毒素大肠杆菌结肠炎住院后出现5个月腹泻史和体重减轻40磅。患者既往有明显的结肠镜检查史,发现有数百个息肉,父亲在45岁时死于结直肠癌。多次重复感染性粪便检查均为阴性,抗生素未能解决患者的症状。患者行内窥镜检查,发现从直肠到回肠末端有大量息肉,与假性息肉相似,可能为炎症性肠病。随后的组织学显示表面糜烂和炎症,但没有发育不良。内窥镜检查显示炎性息肉伴纤维蛋白脓性粘液。在没有慢性炎症的情况下(住院后c反应蛋白在正常范围内),内镜和组织学结果提示帽息肉病综合征。结论:帽状息肉病可通过内镜和组织学诊断。虽然大多数帽息肉病的病例局限于远端结肠和直肠,但我们认为这是第一例帽息肉病综合征延伸到回肠末端。帽息肉病综合征的治疗取决于症状的严重程度。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


