{"title":"Trigeminal Neuralgia as a Rare Complication of Idiopathic Intracranial Hypertension.","authors":"Mariana Sarov-Riviere, Claire Ancelet, Ghaidaa Nasser, Jildaz Caroff, Nozar Aghakhani, Christian Denier","doi":"10.1159/000544077","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Idiopathic intracranial hypertension (IIH) is a rare cause of chronic headaches. Usually, patients with IIH present headaches and papilledema with no focal neurological signs. Classical MRI findings feature characteristic signs, i.e., dilated perioptic nerves sheath and empty sella turcica. Rarely, cranial nerve palsies existed, especially abducens nerve palsy.</p><p><strong>Case presentation: </strong>We reported herein another rare clinical feature of IIH: trigeminal neuralgia in association with meningocele. This 35-year-old obese woman initially presented with chronic headaches and papilledema. Cerebral MRI showed classical IIH findings. The CSF opening pressure was increased. A treatment coupling acetazolamide and iterative lumbar punctures led to the regression of papilledema, but headaches were difficult to control. Ten years later, while she was lost to follow up and treated with acetazolamide by her <i>general practitioner</i>, she developed extremely painful neuropathic pain in the left trigeminal nerve territory, in association with a recurrence of the chronic headaches. A new MRI showed new bilateral cavum trigeminal meningoceles, predominantly on the left side, associated with an atrophy of the cisternal segment of the left trigeminal nerve. Angio-CT showed transverse sinus stenosis, treated by stenting. After this treatment, IIH symptoms disappeared, while trigeminal neuralgia amplified: a surgical procedure led to its complete disappearance.</p><p><strong>Conclusion: </strong>To our knowledge, this is the first case reported of trigeminal neuralgia associated with meningocele formation in IIH. Our case illustrates the great efficacy of venous stenting in IIH, and one may wonder whether earlier stenting could have avoided the subsequent development of meningoceles and subsequent neuralgia.</p>","PeriodicalId":9639,"journal":{"name":"Case Reports in Neurology","volume":"17 1","pages":"57-61"},"PeriodicalIF":0.6000,"publicationDate":"2025-04-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12068838/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Neurology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000544077","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Idiopathic intracranial hypertension (IIH) is a rare cause of chronic headaches. Usually, patients with IIH present headaches and papilledema with no focal neurological signs. Classical MRI findings feature characteristic signs, i.e., dilated perioptic nerves sheath and empty sella turcica. Rarely, cranial nerve palsies existed, especially abducens nerve palsy.
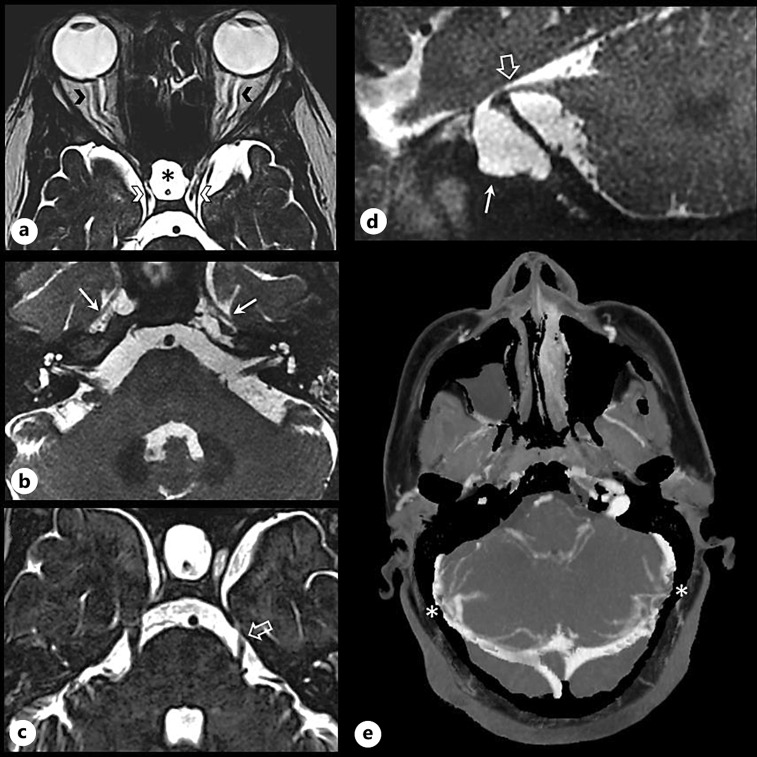
Case presentation: We reported herein another rare clinical feature of IIH: trigeminal neuralgia in association with meningocele. This 35-year-old obese woman initially presented with chronic headaches and papilledema. Cerebral MRI showed classical IIH findings. The CSF opening pressure was increased. A treatment coupling acetazolamide and iterative lumbar punctures led to the regression of papilledema, but headaches were difficult to control. Ten years later, while she was lost to follow up and treated with acetazolamide by her general practitioner, she developed extremely painful neuropathic pain in the left trigeminal nerve territory, in association with a recurrence of the chronic headaches. A new MRI showed new bilateral cavum trigeminal meningoceles, predominantly on the left side, associated with an atrophy of the cisternal segment of the left trigeminal nerve. Angio-CT showed transverse sinus stenosis, treated by stenting. After this treatment, IIH symptoms disappeared, while trigeminal neuralgia amplified: a surgical procedure led to its complete disappearance.
Conclusion: To our knowledge, this is the first case reported of trigeminal neuralgia associated with meningocele formation in IIH. Our case illustrates the great efficacy of venous stenting in IIH, and one may wonder whether earlier stenting could have avoided the subsequent development of meningoceles and subsequent neuralgia.
期刊介绍:
This new peer-reviewed online-only journal publishes original case reports covering the entire spectrum of neurology. Clinicians and researchers are given a tool to disseminate their personal experience to a wider public as well as to review interesting cases encountered by colleagues all over the world. To complement the contributions supplementary material is welcomed. The reports are searchable according to the key words supplied by the authors; it will thus be possible to search across the entire growing collection of case reports with universally used terms, further facilitating the retrieval of specific information. Following the open access principle, the entire contents can be retrieved at no charge, guaranteeing easy access to this valuable source of anecdotal information at all times.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


