Witold Streb, Roland Fiszer, Katarzyna Mitręga, Tomasz Podolecki, Tomasz Kurek, Monika Lazar, Wiktoria Kowalska, Anna Wizner, Anita Stanjek-Cichoracka, Zbigniew Kalarus
{"title":"Optimizing MitraClip Outcomes: The Case for Routine Iatrogenic ASD Closure.","authors":"Witold Streb, Roland Fiszer, Katarzyna Mitręga, Tomasz Podolecki, Tomasz Kurek, Monika Lazar, Wiktoria Kowalska, Anna Wizner, Anita Stanjek-Cichoracka, Zbigniew Kalarus","doi":"10.1177/11795468251332236","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Iatrogenic atrial septal defect (iASD) resulting from MitraClip procedures may cause volume overload and deterioration of right ventricular (RV) function. The concurrent MitraClip procedure, along with an intervention to close iASD appears to yield a potentially favorable impact on the functioning of the right ventricle.</p><p><strong>Aim of the study: </strong>The study aims to evaluate the effect of iASD closure with an occluder immediately after the MitraClip procedure on RV function, pulmonary resistance, and right ventricle-pulmonary artery coupling (RV-PAc).</p><p><strong>Methods: </strong>The study group (ASDc) consisted of consecutive patients who underwent concomitant iASD closure with the Amplatzer occluder (n = 10). The control group (n = 9) comprised patients with iASD left untreated (CT group). RV assessment before MitraClip and during follow-up visits was based on transthoracic echocardiography (TTE).</p><p><strong>Results: </strong>In the CT group, fractional area change (FAC) increased from 33.3 ± 15.6% to 38.2 ± 14.0%; <i>P</i> = .28, and in the ASDc group, from 38.9 ± 11.6% to 40.4 ± 13.7%; <i>P</i> = .76. In the CT group, tricuspid annular plane systolic excursion (TAPSE) decreased from 19.2 ± 4.3 mm to 17.3 ± 3.8 mm; <i>P</i> = .47, and in the ASDc group from 19.1 ± 6.8 mm to 16.5 ± 6.1 mm; <i>P</i> = .04. In the entire group, right ventricular systolic pressure (RVSP) dropped from 52.7 ± 16.0 mmHg to 45.1 ± 8.1 mmHg; <i>P</i> = .01. The reduction in RVSP was 11 mmHg in the ASDc group versus 4 mmHg in the CT group (<i>P</i> = .35). Pulmonary vascular resistance (PVR) itself did not change significantly before and after the procedure. RV-PAc increased respectively by 36% and 9.75% from baseline values in the ASDc and CT groups.</p><p><strong>Conclusion: </strong>Closure of the iASD results in a greater reduction in RVSP but also TAPSE. RV-PAc, a parameter unaffected by RV preload, reveals notably improved hemodynamic conditions for RV performance after iASD closure.</p>","PeriodicalId":10419,"journal":{"name":"Clinical Medicine Insights. Cardiology","volume":"19 ","pages":"11795468251332236"},"PeriodicalIF":3.3000,"publicationDate":"2025-04-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12033620/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795468251332236","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Iatrogenic atrial septal defect (iASD) resulting from MitraClip procedures may cause volume overload and deterioration of right ventricular (RV) function. The concurrent MitraClip procedure, along with an intervention to close iASD appears to yield a potentially favorable impact on the functioning of the right ventricle.
Aim of the study: The study aims to evaluate the effect of iASD closure with an occluder immediately after the MitraClip procedure on RV function, pulmonary resistance, and right ventricle-pulmonary artery coupling (RV-PAc).
Methods: The study group (ASDc) consisted of consecutive patients who underwent concomitant iASD closure with the Amplatzer occluder (n = 10). The control group (n = 9) comprised patients with iASD left untreated (CT group). RV assessment before MitraClip and during follow-up visits was based on transthoracic echocardiography (TTE).
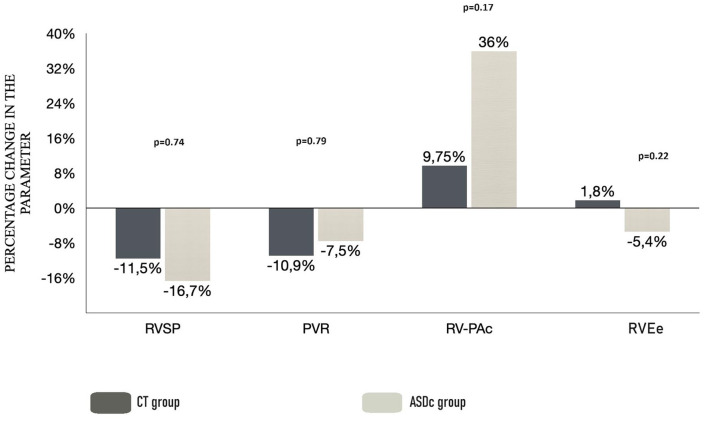
Results: In the CT group, fractional area change (FAC) increased from 33.3 ± 15.6% to 38.2 ± 14.0%; P = .28, and in the ASDc group, from 38.9 ± 11.6% to 40.4 ± 13.7%; P = .76. In the CT group, tricuspid annular plane systolic excursion (TAPSE) decreased from 19.2 ± 4.3 mm to 17.3 ± 3.8 mm; P = .47, and in the ASDc group from 19.1 ± 6.8 mm to 16.5 ± 6.1 mm; P = .04. In the entire group, right ventricular systolic pressure (RVSP) dropped from 52.7 ± 16.0 mmHg to 45.1 ± 8.1 mmHg; P = .01. The reduction in RVSP was 11 mmHg in the ASDc group versus 4 mmHg in the CT group (P = .35). Pulmonary vascular resistance (PVR) itself did not change significantly before and after the procedure. RV-PAc increased respectively by 36% and 9.75% from baseline values in the ASDc and CT groups.
Conclusion: Closure of the iASD results in a greater reduction in RVSP but also TAPSE. RV-PAc, a parameter unaffected by RV preload, reveals notably improved hemodynamic conditions for RV performance after iASD closure.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


