Michael R Zile, William T Abraham, Lynne W Stevenson, Maria Rosa Costanzo, Christiane E Angermann, Mandeep R Mehra, Akshay S Desai, Anique Ducharme, Nessa Johnson, John Henderson, JoAnn Lindenfeld
{"title":"Relationship Between Remote, Ambulatory Pulmonary Artery Pressures, and All-Cause Mortality in Patients With Chronic Heart Failure.","authors":"Michael R Zile, William T Abraham, Lynne W Stevenson, Maria Rosa Costanzo, Christiane E Angermann, Mandeep R Mehra, Akshay S Desai, Anique Ducharme, Nessa Johnson, John Henderson, JoAnn Lindenfeld","doi":"10.1161/CIRCHEARTFAILURE.124.012754","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hemodynamically guided management of patients with chronic heart failure (HF), using a remote, ambulatory pulmonary artery (PA) pressure monitor, has been shown to reduce mortality and morbidity. These improved outcomes were associated with a reduction in PA pressure. However, several pivotal questions remain unanswered: do systolic, diastolic, or mean PA pressures each predict all-cause mortality? Do PA pressures predict mortality across the ejection fraction (EF) spectrum? Do increases or decreases in PA pressure over time predict increases or decreases in mortality?</p><p><strong>Methods: </strong>Retrospective analyses of data from CHAMPION (CardioMEMS Heart Sensor Allows Monitoring of Pressure to Improve Outcomes in NYHA Class III Heart Failure Patients; n=550), GUIDE-HF (Hemodynamic-GUIDEed management of Heart Failure; n=2358), US PAS (CardioMEMS HF System Post Approval Study; n=1200), and MEMS-HF (CardioMEMS Monitoring Study for Heart Failure; n=234) were performed, including all enrolled patients regardless of treatment assignments (Total N=4342). PA systolic, PA diastolic, and PA mean pressures were examined in patients with HF and reduced EF (<50%, n=2562) and preserved EF (≥50%, n=1454). Baseline pressure (averaged over 14 days after implantation) and change in pressure (increase/decrease/no change) from baseline to 6 months (averaged over 14 days just before the 6-month time point) were related to all-cause mortality over a 2-year follow-up period.</p><p><strong>Results: </strong>Baseline PA diastolic, independent of other covariates, was a significant predictor of mortality (hazard ratio, 1.04 [95% CI, 1.03-1.05]; <i>P</i><0.0001). Change in PA diastolic from baseline to 6 months (assessed as a continuous variable) was an independent predictor of mortality after 6 months (landmark analysis; hazard ratio, 1.03 [95% CI, 1.01-1.05]; <i>P</i>=0.0042). Change in PA diastolic from baseline to 6 months(assessed as a categorical variable) decrease or increase of >2 mm Hg compared with no change predicted a 14.7% decrease and 26.7% increase in mortality, respectively (<i>P</i>=0.0237). PA systolic and PA mean pressures in both HF with reduced EF and HF with preserved EF patients, for both baseline and change from baseline to 6 months, were also predictive of all-cause mortality.</p><p><strong>Conclusions: </strong>Baseline PAP (systolic, diastolic, and mean) and change in PAP (systolic, diastolic, and mean) from baseline to 6 months were independent predictors of 2-year mortality in patients with chronic HF in both preserved and reduced EF.</p><p><strong>Registration: </strong>URL: https://www.clinicaltrials.gov; Unique identifiers: CHAMPION, NCT00531661; GUIDE-HF, NCT03387813; USPAS, NCT02279888; MEMS-HF, NCT02693691.</p>","PeriodicalId":10196,"journal":{"name":"Circulation: Heart Failure","volume":" ","pages":"e012754"},"PeriodicalIF":8.4000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12165488/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Circulation: Heart Failure","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1161/CIRCHEARTFAILURE.124.012754","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/14 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
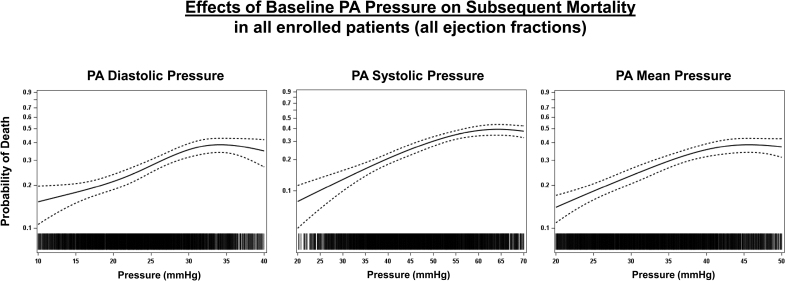
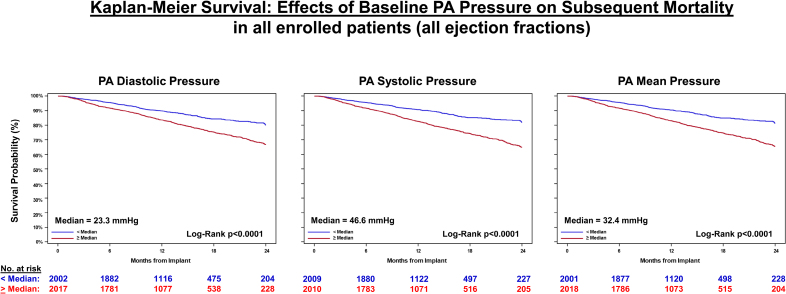
Background: Hemodynamically guided management of patients with chronic heart failure (HF), using a remote, ambulatory pulmonary artery (PA) pressure monitor, has been shown to reduce mortality and morbidity. These improved outcomes were associated with a reduction in PA pressure. However, several pivotal questions remain unanswered: do systolic, diastolic, or mean PA pressures each predict all-cause mortality? Do PA pressures predict mortality across the ejection fraction (EF) spectrum? Do increases or decreases in PA pressure over time predict increases or decreases in mortality?
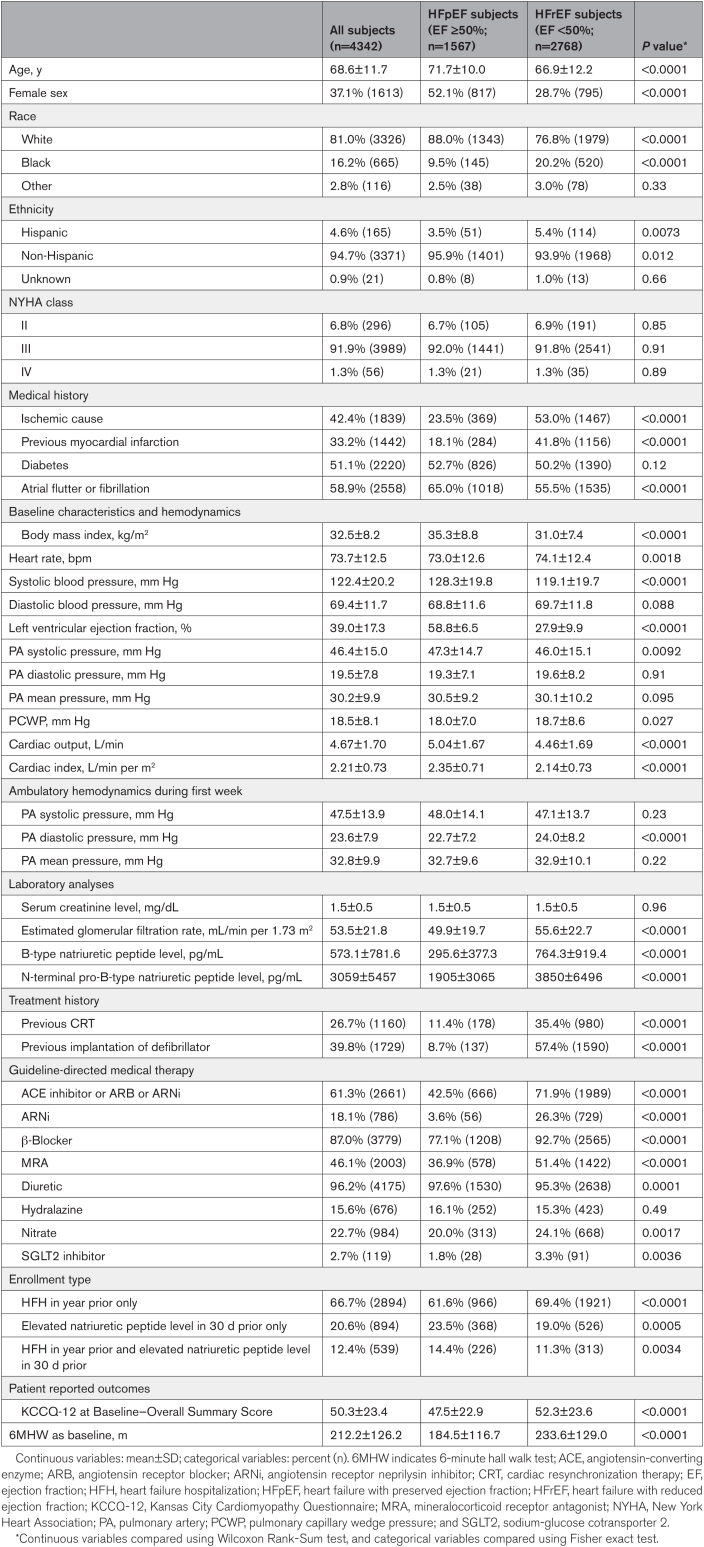
Methods: Retrospective analyses of data from CHAMPION (CardioMEMS Heart Sensor Allows Monitoring of Pressure to Improve Outcomes in NYHA Class III Heart Failure Patients; n=550), GUIDE-HF (Hemodynamic-GUIDEed management of Heart Failure; n=2358), US PAS (CardioMEMS HF System Post Approval Study; n=1200), and MEMS-HF (CardioMEMS Monitoring Study for Heart Failure; n=234) were performed, including all enrolled patients regardless of treatment assignments (Total N=4342). PA systolic, PA diastolic, and PA mean pressures were examined in patients with HF and reduced EF (<50%, n=2562) and preserved EF (≥50%, n=1454). Baseline pressure (averaged over 14 days after implantation) and change in pressure (increase/decrease/no change) from baseline to 6 months (averaged over 14 days just before the 6-month time point) were related to all-cause mortality over a 2-year follow-up period.
Results: Baseline PA diastolic, independent of other covariates, was a significant predictor of mortality (hazard ratio, 1.04 [95% CI, 1.03-1.05]; P<0.0001). Change in PA diastolic from baseline to 6 months (assessed as a continuous variable) was an independent predictor of mortality after 6 months (landmark analysis; hazard ratio, 1.03 [95% CI, 1.01-1.05]; P=0.0042). Change in PA diastolic from baseline to 6 months(assessed as a categorical variable) decrease or increase of >2 mm Hg compared with no change predicted a 14.7% decrease and 26.7% increase in mortality, respectively (P=0.0237). PA systolic and PA mean pressures in both HF with reduced EF and HF with preserved EF patients, for both baseline and change from baseline to 6 months, were also predictive of all-cause mortality.
Conclusions: Baseline PAP (systolic, diastolic, and mean) and change in PAP (systolic, diastolic, and mean) from baseline to 6 months were independent predictors of 2-year mortality in patients with chronic HF in both preserved and reduced EF.
期刊介绍:
Circulation: Heart Failure focuses on content related to heart failure, mechanical circulatory support, and heart transplant science and medicine. It considers studies conducted in humans or analyses of human data, as well as preclinical studies with direct clinical correlation or relevance. While primarily a clinical journal, it may publish novel basic and preclinical studies that significantly advance the field of heart failure.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


