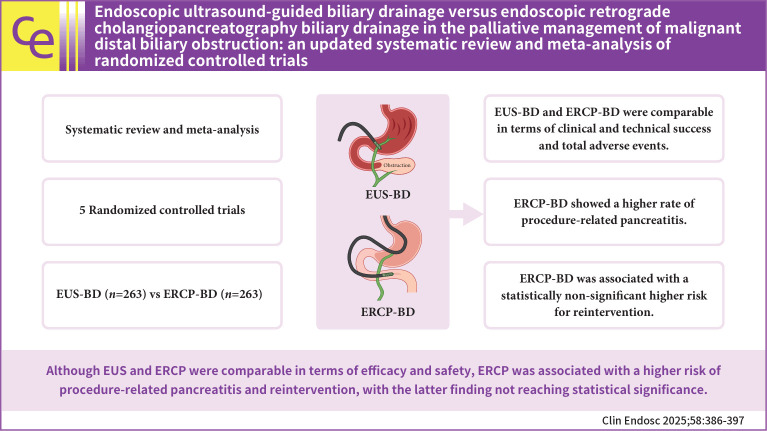
Endoscopic ultrasound-guided biliary drainage versus endoscopic retrograde cholangiopancreatography biliary drainage in the palliative management of malignant distal biliary obstruction: an updated systematic review and meta-analysis of randomized controlled trials.
Spyros Peppas, Advait Suvarnakar, Bara A Abujaber, Nadera Altork, Amer Arman, Sayel Alzraikat, Akram I Ahmad, Camille Boustani, Won Kyoo Cho
{"title":"Endoscopic ultrasound-guided biliary drainage versus endoscopic retrograde cholangiopancreatography biliary drainage in the palliative management of malignant distal biliary obstruction: an updated systematic review and meta-analysis of randomized controlled trials.","authors":"Spyros Peppas, Advait Suvarnakar, Bara A Abujaber, Nadera Altork, Amer Arman, Sayel Alzraikat, Akram I Ahmad, Camille Boustani, Won Kyoo Cho","doi":"10.5946/ce.2024.155","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/aims: </strong>Evidence suggests comparable outcomes between endoscopic ultrasound (EUS) and endoscopic retrograde cholangiopancreatography (ERCP) in the biliary drainage of malignant distal biliary obstruction (MDBO). We conducted an updated systematic review and meta-analysis comparing the EUS with ERCP in the management of MDBO.</p><p><strong>Methods: </strong>We performed a literature search using the Medline, Embase and Cochrane databases, including randomized controlled trials comparing EUS and ERCP in patients with MDBO. Meta-analysis was performed using the random-effects model using the STATA ver. 17.0 software.</p><p><strong>Results: </strong>Both procedures were comparable in technical (risk ratio [RR], 1.01; 95% confidence interval [CI], 0.78-1.30) and clinical (RR, 1.10; 95% CI, 0.85-1.41) success. No difference was identified in total adverse events (RR, 0.75; 95% CI, 0.42-1.35), acute cholangitis (RR, 0.84; 95% CI, 0.43-1.62), stent patency (RR, 1.13; 95% CI, 0.87-1.46) and mean stent patency time (mean difference, -0.01; 95% CI: -0.21 to 0.19). ERCP was associated with a higher risk of procedure-related pancreatitis (RR, 0.17; 95% CI, 0.04-0.68) and statistically non-significant higher risk for reintervention (RR, 0.61; 95% CI, 0.37-1.01).</p><p><strong>Conclusions: </strong>Although EUS and ERCP were comparable in terms of efficacy and safety, ERCP was associated with a higher risk of procedure-related pancreatitis and reintervention, with the latter finding not reaching statistical significance.</p>","PeriodicalId":10351,"journal":{"name":"Clinical Endoscopy","volume":" ","pages":"386-397"},"PeriodicalIF":2.3000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12138357/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Endoscopy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5946/ce.2024.155","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/9 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
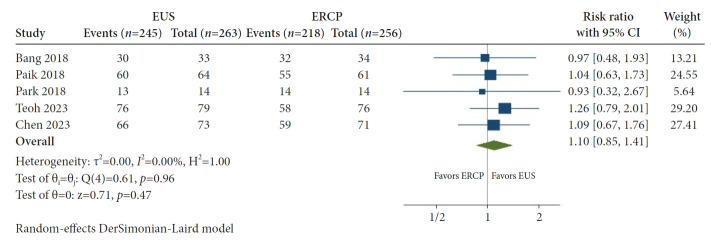
Background/aims: Evidence suggests comparable outcomes between endoscopic ultrasound (EUS) and endoscopic retrograde cholangiopancreatography (ERCP) in the biliary drainage of malignant distal biliary obstruction (MDBO). We conducted an updated systematic review and meta-analysis comparing the EUS with ERCP in the management of MDBO.
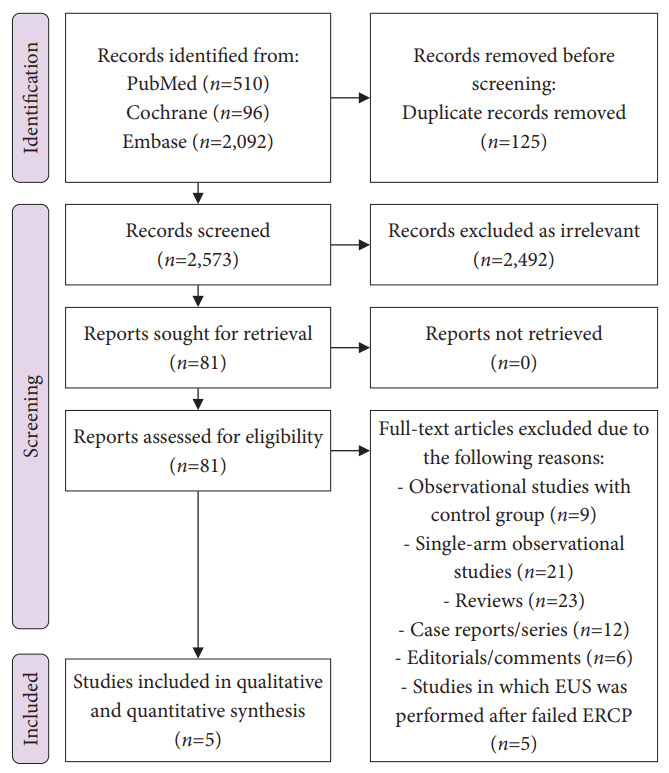
Methods: We performed a literature search using the Medline, Embase and Cochrane databases, including randomized controlled trials comparing EUS and ERCP in patients with MDBO. Meta-analysis was performed using the random-effects model using the STATA ver. 17.0 software.
Results: Both procedures were comparable in technical (risk ratio [RR], 1.01; 95% confidence interval [CI], 0.78-1.30) and clinical (RR, 1.10; 95% CI, 0.85-1.41) success. No difference was identified in total adverse events (RR, 0.75; 95% CI, 0.42-1.35), acute cholangitis (RR, 0.84; 95% CI, 0.43-1.62), stent patency (RR, 1.13; 95% CI, 0.87-1.46) and mean stent patency time (mean difference, -0.01; 95% CI: -0.21 to 0.19). ERCP was associated with a higher risk of procedure-related pancreatitis (RR, 0.17; 95% CI, 0.04-0.68) and statistically non-significant higher risk for reintervention (RR, 0.61; 95% CI, 0.37-1.01).
Conclusions: Although EUS and ERCP were comparable in terms of efficacy and safety, ERCP was associated with a higher risk of procedure-related pancreatitis and reintervention, with the latter finding not reaching statistical significance.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


