Yang Sun, Zexu Chen, Yan Liu, Qiuyi Huo, Wan-Nan Jia, Zhennan Zhao, Tianhui Chen, Yongxiang Jiang
{"title":"Novel classification for microspherophakia and its related surgical implications: a retrospective cohort study.","authors":"Yang Sun, Zexu Chen, Yan Liu, Qiuyi Huo, Wan-Nan Jia, Zhennan Zhao, Tianhui Chen, Yongxiang Jiang","doi":"10.1136/bmjophth-2024-002063","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A novel classification for microspherophakia (MSP) was developed using a nomogram model to stratify patients and evaluate surgical outcomes.</p><p><strong>Methods: </strong>The study involved 99 eyes from 64 MSP patients, divided into training (64 eyes) and validation (35 eyes) cohorts. Primary outcome included the best corrected distance visual acuity (BCVA) at the 1-year follow-up, and the secondary outcome was intraocular pressure (IOP) control. MSP patients achieving a BCVA of ≤0.2 logarithm of the minimal angle of resolution with successful IOP control were categorised into the favourable outcomes group, while those not meeting these criteria were placed in the unfavourable outcomes group. A nomogram model was constructed to predict unfavourable outcomes by identifying associated risk factors.</p><p><strong>Results: </strong>In the training cohort, 39.06% (25/64) achieved favourable outcomes, while 60.94% (39/64) had unfavourable outcomes. Decreased anterior chamber depth (ACD) and the presence of glaucoma were identified as risk factors for predicting unfavourable outcomes. The concordance index for the training and validation cohorts was 0.828 and 0.768, respectively. A nomogram-derived cut-off value of 56 points stratified patients into low-risk (≤56 points) and high-risk (>56 points) groups. Postoperative BCVA was significantly better in the low-risk group at 6-month and 1-year follow-ups.</p><p><strong>Conclusion: </strong>MSP patients in the low-risk group achieved satisfactory outcomes. For high-risk patients with shallowing ACD, early surgical intervention is recommended to prevent secondary glaucoma. Close monitoring of IOP and glaucoma progression is crucial for patients with secondary glaucoma. This classification offers valuable insights for outcome stratification and guidance in clinical decision-making for MSP management. However, the limitations of this study include its small sample size, which may impact generalisability, and future studies with larger cohorts are needed to validate and refine the nomogram.</p>","PeriodicalId":9286,"journal":{"name":"BMJ Open Ophthalmology","volume":"10 1","pages":""},"PeriodicalIF":2.2000,"publicationDate":"2025-05-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12049971/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Ophthalmology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjophth-2024-002063","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"OPHTHALMOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: A novel classification for microspherophakia (MSP) was developed using a nomogram model to stratify patients and evaluate surgical outcomes.
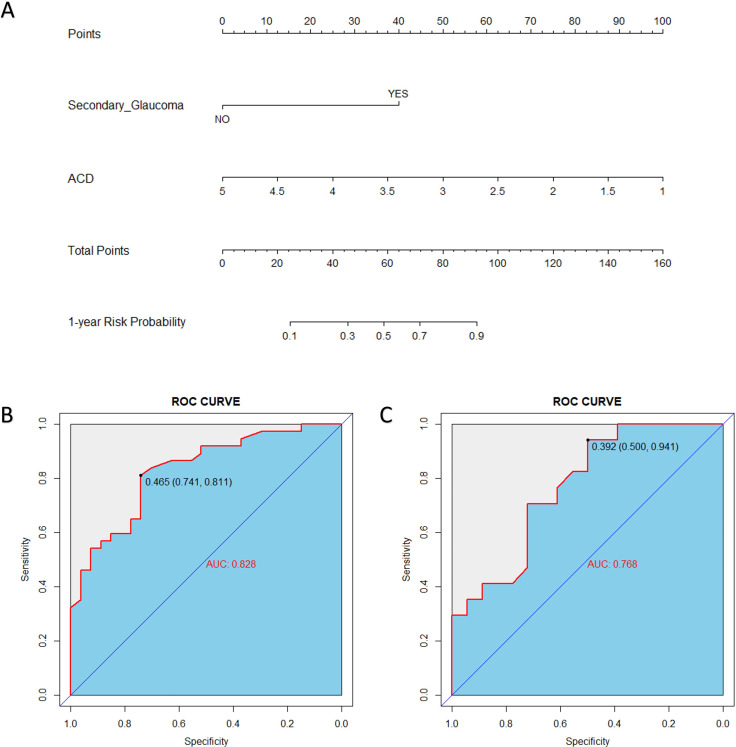
Methods: The study involved 99 eyes from 64 MSP patients, divided into training (64 eyes) and validation (35 eyes) cohorts. Primary outcome included the best corrected distance visual acuity (BCVA) at the 1-year follow-up, and the secondary outcome was intraocular pressure (IOP) control. MSP patients achieving a BCVA of ≤0.2 logarithm of the minimal angle of resolution with successful IOP control were categorised into the favourable outcomes group, while those not meeting these criteria were placed in the unfavourable outcomes group. A nomogram model was constructed to predict unfavourable outcomes by identifying associated risk factors.
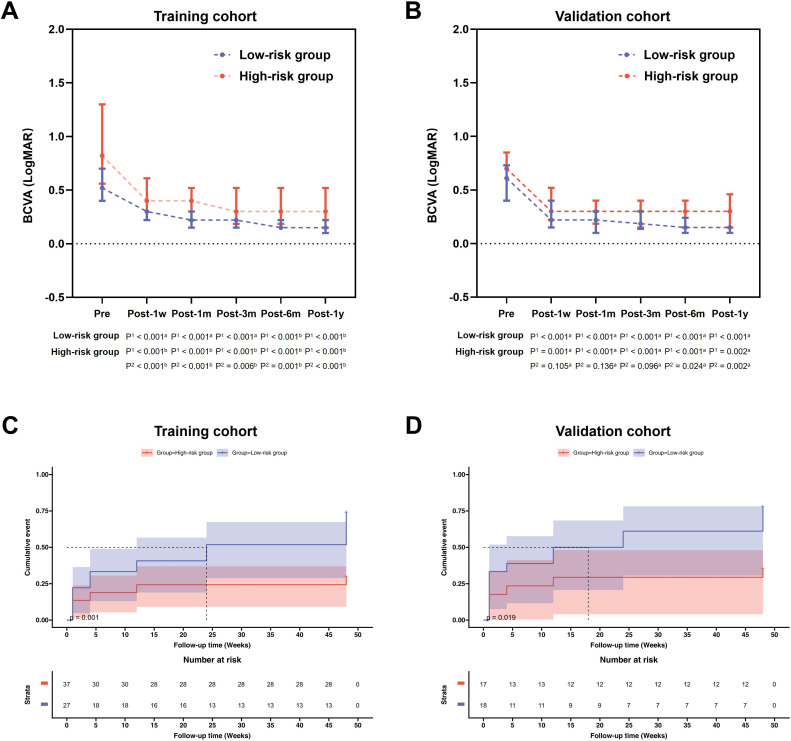
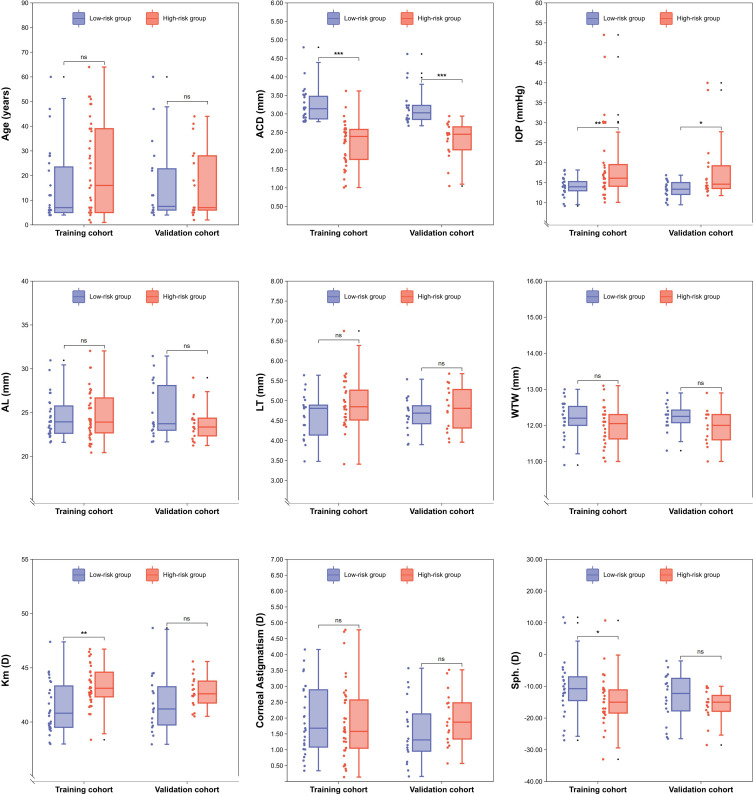
Results: In the training cohort, 39.06% (25/64) achieved favourable outcomes, while 60.94% (39/64) had unfavourable outcomes. Decreased anterior chamber depth (ACD) and the presence of glaucoma were identified as risk factors for predicting unfavourable outcomes. The concordance index for the training and validation cohorts was 0.828 and 0.768, respectively. A nomogram-derived cut-off value of 56 points stratified patients into low-risk (≤56 points) and high-risk (>56 points) groups. Postoperative BCVA was significantly better in the low-risk group at 6-month and 1-year follow-ups.
Conclusion: MSP patients in the low-risk group achieved satisfactory outcomes. For high-risk patients with shallowing ACD, early surgical intervention is recommended to prevent secondary glaucoma. Close monitoring of IOP and glaucoma progression is crucial for patients with secondary glaucoma. This classification offers valuable insights for outcome stratification and guidance in clinical decision-making for MSP management. However, the limitations of this study include its small sample size, which may impact generalisability, and future studies with larger cohorts are needed to validate and refine the nomogram.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


