Chronic Liver Disease Primarily Presenting with Motor Weakness by Intractable Hypokalemia with Combined Respiratory Alkalosis and Chronic Diarrhea: A Case Report.
{"title":"Chronic Liver Disease Primarily Presenting with Motor Weakness by Intractable Hypokalemia with Combined Respiratory Alkalosis and Chronic Diarrhea: A Case Report.","authors":"Nam-Seon Beck, Yeon-Oh Jeong, Kyung-Hee Lee, Eun-Mi Jun, Joung-Il Im, Sae-Yong Hong","doi":"10.1159/000544099","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Most patients with compensated cirrhosis remain asymptomatic. However, with the onset of decompensation, electrolyte and acid-base disturbances are frequent in patients with chronic liver disease, including hypokalemia. We encountered a case of chronic liver disease with portal hypertension, primarily presenting with motor weakness caused by intractable hypokalemia, hypoxia-associated respiratory alkalosis, and chronic diarrhea.</p><p><strong>Case presentation: </strong>A 54-year-old male presented to the emergency department with motor weakness. He reported experiencing exertional dyspnea and watery diarrhea for the past 3 months, approximately ten times daily. Arterial blood gas analysis indicated hypoxia and hypocapnia compatible with chronic respiratory alkalosis. The transtubular potassium gradient was 1.69, and the aldosterone/renin ratio was 17.6 (ng/dL)/(ng/mL/h). The patient had a 30-year history of consuming 360-720 mL of 20% alcohol almost daily. Abdominal computed tomography revealed multiple regenerative and dysplastic nodules in the liver, splenomegaly, ascites, esophageal varices, and diffuse edematous wall thickening in the bowel, suggesting portal hypertensive enteropathy. Computed tomography of the lungs showed no specific abnormalities in the lungs, pleura, or thoracic wall.</p><p><strong>Conclusion: </strong>We present a case of liver cirrhosis complicated by intractable hypokalemia, respiratory alkalosis, portal hypertension, and chronic diarrhea. A 24-h urine analysis showed renal excretion levels of Na<sup>+</sup>, K<sup>+</sup>, and Cl<sup>-</sup> at 6.0, 2.5, and 11.0 mmol, respectively, suggesting renal retention of these electrolytes. Meanwhile, the serum levels of Na<sup>+</sup>, K<sup>+</sup>, and Cl<sup>-</sup> were 136, 1.8, and 98 mEq/L, respectively, indicating a preserved balance of sodium and chloride but not potassium. This case underscores the importance of clinicians considering both liver cirrhosis-associated hypoxia and chronic liver disease-induced chronic diarrhea as potential underlying causes, especially when more common causes of hypokalemia have been excluded.</p>","PeriodicalId":9614,"journal":{"name":"Case Reports in Gastroenterology","volume":"19 1","pages":"165-172"},"PeriodicalIF":0.6000,"publicationDate":"2025-03-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11913463/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000544099","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Most patients with compensated cirrhosis remain asymptomatic. However, with the onset of decompensation, electrolyte and acid-base disturbances are frequent in patients with chronic liver disease, including hypokalemia. We encountered a case of chronic liver disease with portal hypertension, primarily presenting with motor weakness caused by intractable hypokalemia, hypoxia-associated respiratory alkalosis, and chronic diarrhea.
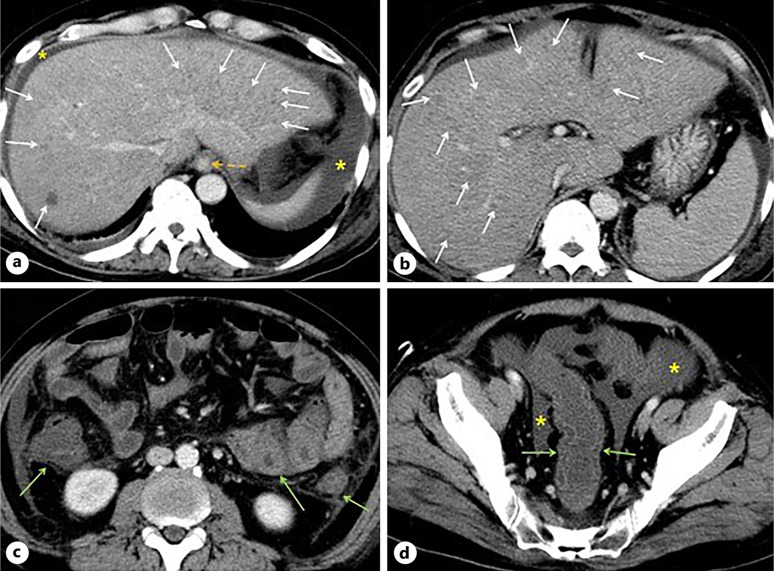
Case presentation: A 54-year-old male presented to the emergency department with motor weakness. He reported experiencing exertional dyspnea and watery diarrhea for the past 3 months, approximately ten times daily. Arterial blood gas analysis indicated hypoxia and hypocapnia compatible with chronic respiratory alkalosis. The transtubular potassium gradient was 1.69, and the aldosterone/renin ratio was 17.6 (ng/dL)/(ng/mL/h). The patient had a 30-year history of consuming 360-720 mL of 20% alcohol almost daily. Abdominal computed tomography revealed multiple regenerative and dysplastic nodules in the liver, splenomegaly, ascites, esophageal varices, and diffuse edematous wall thickening in the bowel, suggesting portal hypertensive enteropathy. Computed tomography of the lungs showed no specific abnormalities in the lungs, pleura, or thoracic wall.
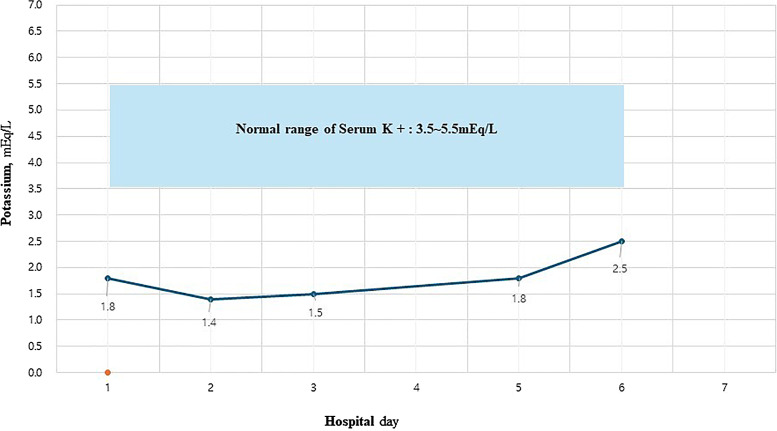
Conclusion: We present a case of liver cirrhosis complicated by intractable hypokalemia, respiratory alkalosis, portal hypertension, and chronic diarrhea. A 24-h urine analysis showed renal excretion levels of Na+, K+, and Cl- at 6.0, 2.5, and 11.0 mmol, respectively, suggesting renal retention of these electrolytes. Meanwhile, the serum levels of Na+, K+, and Cl- were 136, 1.8, and 98 mEq/L, respectively, indicating a preserved balance of sodium and chloride but not potassium. This case underscores the importance of clinicians considering both liver cirrhosis-associated hypoxia and chronic liver disease-induced chronic diarrhea as potential underlying causes, especially when more common causes of hypokalemia have been excluded.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


