{"title":"Optimal Systolic Blood Pressure Control After Thrombectomy in Acute Ischemic Stroke: A Systematic Review and Meta-analysis.","authors":"Baikuntha Panigrahi, Rohit Bhatia, Partha Haldar, Risha Sarkar, Imnameren Longkumer","doi":"10.4103/aian.aian_1087_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>The optimal systolic blood pressure (SBP) control after endovascular thrombectomy (EVT) is unclear. This study aimed to determine whether intensive SBP control (<140 mmHg) within 24 h post-EVT, compared to conventional management (<180 mmHg), leads to a better functional outcome, defined as a modified Rankin Scale (mRS) score of 0-2 at 90 days.</p><p><strong>Methods: </strong>Following Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines, we searched databases (PubMed, Scopus, EMBASE, Google Scholar, Web of Science) for English language articles up to March 15, 2024. We included randomized controlled trials (RCTs) and observational studies comparing intensive versus conventional SBP control up to 24 h post-EVT. Studies without separate primary outcome data and case series/reports were excluded. The primary outcome was functional independence (mRS 0-2 at 90 days).</p><p><strong>Results: </strong>Twelve studies (n = 5152 patients; five RCTs and seven observational studies) were included, and a primary analysis of the RCTs, along with a secondary exploratory analysis of the observational studies were conducted. The analysis of RCTs favored conventional control for the primary outcome (risk ratio [RR]- 0.81; 95% confidence interval [CI]- 0.73-0.90; P < 0.0001). Mortality rates (RR- 1.14, 95% CI- 0.89-1.45; P = 0.29) and the risk of symptomatic intracranial hemorrhage (RR- 1.10, 95% CI- 0.77-1.58; P = 0.60) were similar in both groups. The secondary exploratory analysis of observational data favored the intensive arm for the primary outcome (RR- 1.28, 95% CI- 1.17-1.41; P < 0.00001).</p><p><strong>Conclusions: </strong>Our primary analysis of RCTs showed that intensive control was associated with poorer functional outcomes, with no significant impact on mortality rate or the risk of symptomatic intracranial hemorrhage. Although observational studies suggested better outcomes with intensive control, we recommend conventional management based on Level 1 evidence from RCTs.PROSPERO Registration no - CRD42023463173.</p>","PeriodicalId":8036,"journal":{"name":"Annals of Indian Academy of Neurology","volume":" ","pages":"323-332"},"PeriodicalIF":1.8000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12192383/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Indian Academy of Neurology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4103/aian.aian_1087_24","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/7 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and objectives: The optimal systolic blood pressure (SBP) control after endovascular thrombectomy (EVT) is unclear. This study aimed to determine whether intensive SBP control (<140 mmHg) within 24 h post-EVT, compared to conventional management (<180 mmHg), leads to a better functional outcome, defined as a modified Rankin Scale (mRS) score of 0-2 at 90 days.
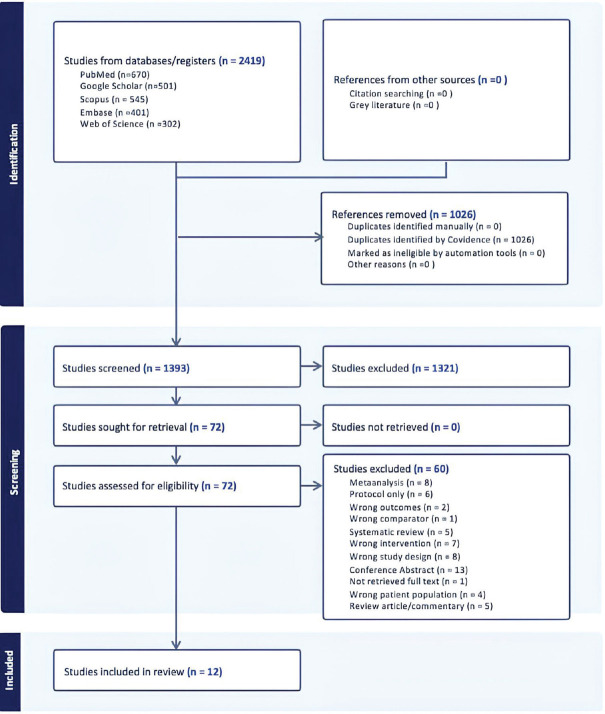
Methods: Following Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines, we searched databases (PubMed, Scopus, EMBASE, Google Scholar, Web of Science) for English language articles up to March 15, 2024. We included randomized controlled trials (RCTs) and observational studies comparing intensive versus conventional SBP control up to 24 h post-EVT. Studies without separate primary outcome data and case series/reports were excluded. The primary outcome was functional independence (mRS 0-2 at 90 days).
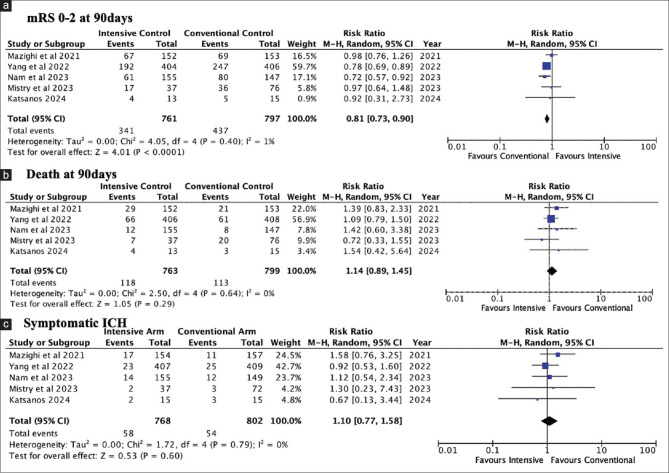
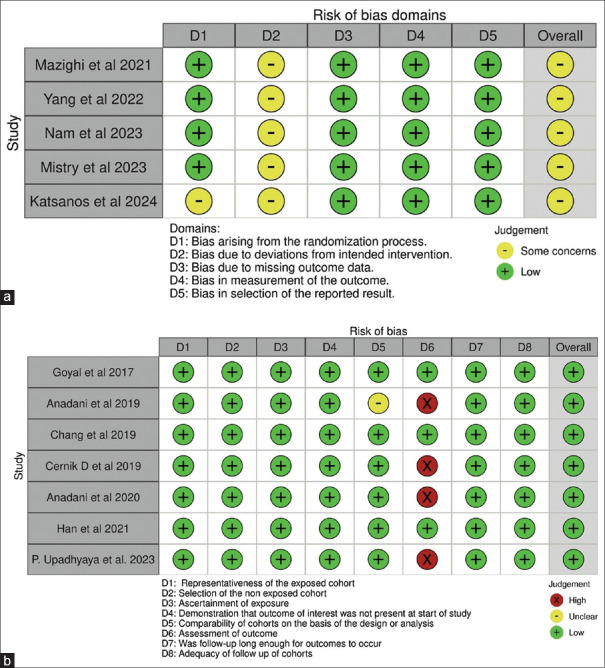
Results: Twelve studies (n = 5152 patients; five RCTs and seven observational studies) were included, and a primary analysis of the RCTs, along with a secondary exploratory analysis of the observational studies were conducted. The analysis of RCTs favored conventional control for the primary outcome (risk ratio [RR]- 0.81; 95% confidence interval [CI]- 0.73-0.90; P < 0.0001). Mortality rates (RR- 1.14, 95% CI- 0.89-1.45; P = 0.29) and the risk of symptomatic intracranial hemorrhage (RR- 1.10, 95% CI- 0.77-1.58; P = 0.60) were similar in both groups. The secondary exploratory analysis of observational data favored the intensive arm for the primary outcome (RR- 1.28, 95% CI- 1.17-1.41; P < 0.00001).
Conclusions: Our primary analysis of RCTs showed that intensive control was associated with poorer functional outcomes, with no significant impact on mortality rate or the risk of symptomatic intracranial hemorrhage. Although observational studies suggested better outcomes with intensive control, we recommend conventional management based on Level 1 evidence from RCTs.PROSPERO Registration no - CRD42023463173.
期刊介绍:
The journal has a clinical foundation and has been utilized most by clinical neurologists for improving the practice of neurology. While the focus is on neurology in India, the journal publishes manuscripts of high value from all parts of the world. Journal publishes reviews of various types, original articles, short communications, interesting images and case reports. The journal respects the scientific submission of its authors and believes in following an expeditious double-blind peer review process and endeavors to complete the review process within scheduled time frame. A significant effort from the author and the journal perhaps enables to strike an equilibrium to meet the professional expectations of the peers in the world of scientific publication. AIAN believes in safeguarding the privacy rights of human subjects. In order to comply with it, the journal instructs all authors when uploading the manuscript to also add the ethical clearance (human/animals)/ informed consent of subject in the manuscript. This applies to the study/case report that involves animal/human subjects/human specimens e.g. extracted tooth part/soft tissue for biopsy/in vitro analysis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


