Sydney Murray, Chance Dumaine, Chris Wall, Tamalina Banerjee, James Barton, Michael Moser
{"title":"Technical and Institutional Factors Affecting Specimen Adequacy and Complications in Ultrasound-guided Kidney Biopsy: A Retrospective Cohort Study.","authors":"Sydney Murray, Chance Dumaine, Chris Wall, Tamalina Banerjee, James Barton, Michael Moser","doi":"10.1177/20543581251336551","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Percutaneous ultrasound-guided kidney biopsy is a critical diagnostic tool with a higher rate of complications than most other biopsies. Our prior research identified technical factors that might improve outcomes.</p><p><strong>Objective: </strong>The objective was to measure the impact of these technical and institutional interventions on specimen adequacy and complication rates in kidney biopsies.</p><p><strong>Design: </strong>This is a retrospective cohort study comparing outcomes before and after intervention implementation.</p><p><strong>Setting: </strong>Two hospitals within a single health region in Saskatchewan serving a population of approximately 1 million.</p><p><strong>Patients: </strong>All adult percutaneous ultrasound-guided kidney biopsies performed on adult patients between 2012 to 2016 (n = 242, pre-implementation) and 2017 to 2021 (n = 338, post-implementation). Both native and transplant biopsies were included, while patients under 18, open biopsies, and biopsies of kidney masses were excluded.</p><p><strong>Measurements: </strong>Primary outcomes included specimen adequacy and biopsy complications (hematoma, hemoglobin drop, infection, and arteriovenous fistula formation).</p><p><strong>Methods: </strong>Technical recommendations included introducing the biopsy needle at a 60° angle, targeting a pole, and avoiding the vascular medulla. Institutional recommendations included microscopic screening for all biopsies, limiting the number of radiologists performing procedures, using a checklist, and restricting computed tomography (CT)-guided biopsies to exceptional cases. Multivariate regression analysis assessed biopsy outcomes before and after the recommendations, controlling for known confounders while at the same time refining factors associated with fewer complications and greater diagnostic yield.</p><p><strong>Results: </strong>The rate of non-diagnostic specimens decreased from 10.3% to 4.4% (<i>P</i> = .005), and complications decreased from 35.5% to 14.2% (<i>P</i> < .0001). Two or three passes yielded excellent diagnostic success, while 4 passes increased the risk of a complication. Multivariate analysis, after accounting for the collinearity of certain technical factors revealed that medulla avoidance and biopsies done after the implementation of the 2016 recommendations significantly reduced the risk of complications (odds ratio [OR] = 0.37, <i>P</i> < .001) and non-diagnostic biopsies (OR = 0.31, <i>P</i> = .002).</p><p><strong>Limitations: </strong>Retrospective design and novelty bias may be a cause of bias in this study. Because the institutional recommendations were followed for all biopsies, it was not possible to distinguish which recommendation was most associated with the improvements. Because our study was done in a single health region, it is not clear if they are generalizable to other programs.</p><p><strong>Conclusions: </strong>The technical and institutional interventions implemented significantly improved specimen adequacy and reduced complication rates in ultrasound-guided kidney biopsies. We have added to these recommendations in that we have refined the requirement for angling the biopsy needle for ease of use and suggest limiting the number of passes to 2 or 3 whenever possible.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"12 ","pages":"20543581251336551"},"PeriodicalIF":1.5000,"publicationDate":"2025-05-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12056320/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581251336551","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Percutaneous ultrasound-guided kidney biopsy is a critical diagnostic tool with a higher rate of complications than most other biopsies. Our prior research identified technical factors that might improve outcomes.
Objective: The objective was to measure the impact of these technical and institutional interventions on specimen adequacy and complication rates in kidney biopsies.
Design: This is a retrospective cohort study comparing outcomes before and after intervention implementation.
Setting: Two hospitals within a single health region in Saskatchewan serving a population of approximately 1 million.
Patients: All adult percutaneous ultrasound-guided kidney biopsies performed on adult patients between 2012 to 2016 (n = 242, pre-implementation) and 2017 to 2021 (n = 338, post-implementation). Both native and transplant biopsies were included, while patients under 18, open biopsies, and biopsies of kidney masses were excluded.
Measurements: Primary outcomes included specimen adequacy and biopsy complications (hematoma, hemoglobin drop, infection, and arteriovenous fistula formation).
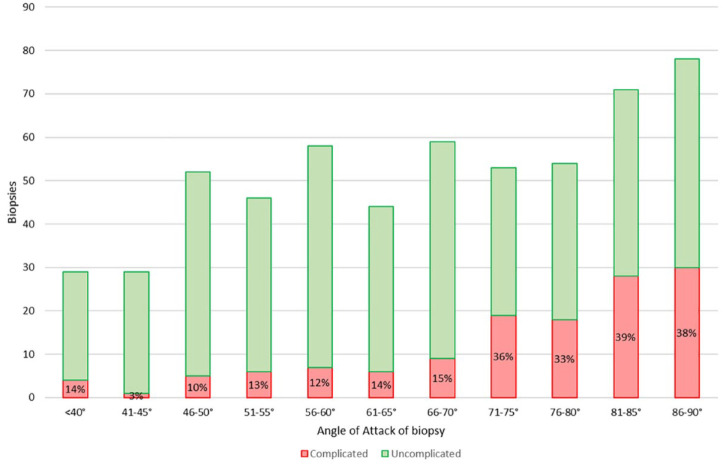
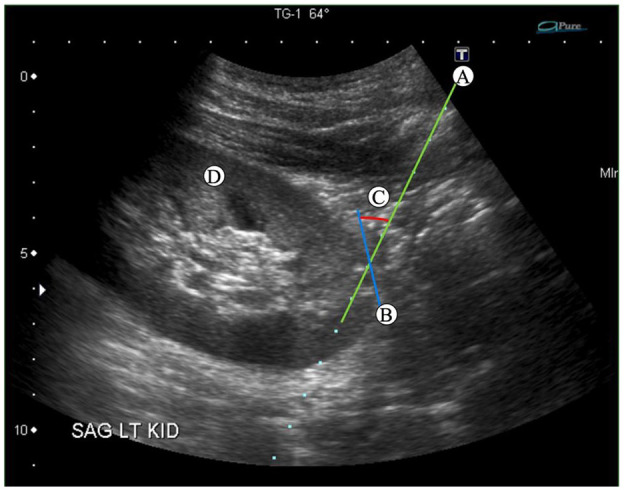
Methods: Technical recommendations included introducing the biopsy needle at a 60° angle, targeting a pole, and avoiding the vascular medulla. Institutional recommendations included microscopic screening for all biopsies, limiting the number of radiologists performing procedures, using a checklist, and restricting computed tomography (CT)-guided biopsies to exceptional cases. Multivariate regression analysis assessed biopsy outcomes before and after the recommendations, controlling for known confounders while at the same time refining factors associated with fewer complications and greater diagnostic yield.
Results: The rate of non-diagnostic specimens decreased from 10.3% to 4.4% (P = .005), and complications decreased from 35.5% to 14.2% (P < .0001). Two or three passes yielded excellent diagnostic success, while 4 passes increased the risk of a complication. Multivariate analysis, after accounting for the collinearity of certain technical factors revealed that medulla avoidance and biopsies done after the implementation of the 2016 recommendations significantly reduced the risk of complications (odds ratio [OR] = 0.37, P < .001) and non-diagnostic biopsies (OR = 0.31, P = .002).
Limitations: Retrospective design and novelty bias may be a cause of bias in this study. Because the institutional recommendations were followed for all biopsies, it was not possible to distinguish which recommendation was most associated with the improvements. Because our study was done in a single health region, it is not clear if they are generalizable to other programs.
Conclusions: The technical and institutional interventions implemented significantly improved specimen adequacy and reduced complication rates in ultrasound-guided kidney biopsies. We have added to these recommendations in that we have refined the requirement for angling the biopsy needle for ease of use and suggest limiting the number of passes to 2 or 3 whenever possible.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


