{"title":"Validation of ARIC heart failure risk score in an Asian population: Results from the CORE-Thailand registry.","authors":"Nichanan Osataphan, Ply Chichareon, Wanwarang Wongcharoen, Krit Leemasawat, Narawudt Prasertwitayakij, Pannipa Suwannasom, Siriluck Gunaparn, Kasem Rattanasumawong, Rungroj Krittayaphong, Arintaya Phrommintikul","doi":"10.1016/j.clinme.2025.100322","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Atherosclerotic Risk in Communities (ARIC) heart failure (HF) score was originally developed in the USA to predict new-onset HF. Our goal was to validate the ARIC-HF score and develop a new score to predict HF in an Asian population.</p><p><strong>Methods: </strong>The Cohort Of patients with high Risk for cardiovascular Events (CORE-Thailand) was a prospective registry of Thai patients with high atherosclerotic risk. Patients were followed for 5 years for HF events. The ARIC-HF score was applied to predict HF. The new ARIC-CORE score was developed by re-estimating the coefficients of ARIC score variables using ridge regression. The discrimination and calibration of the models were assessed. The net reclassification index (NRI) was used to compare the prediction performance between the models. Clinical utility was assessed with a decision curve analysis.</p><p><strong>Results: </strong>From a total of 8,919 patients, 185 (2.1 %) developed HF. The ARIC-HF score and ARIC-CORE HF risk score provided good discrimination with C-statistics of 0.710, (95 % confidence interval (CI); 0.673-0.747) and 0.75, (95 % CI; 0.715-0.785), respectively. Both models showed a good calibration. Using the ARIC-CORE HF score was associated with an improved reclassification of HF (NRI 0.369, 95 % CI; 0.286-0.551) compared to the ARIC-HF score. The net clinical benefit of the ARIC-CORE HF score was higher than the ARIC-HF score in the decision curve analysis.</p><p><strong>Conclusion: </strong>The ARIC-HF score performed well in predicting heart failure in the CORE population. The ARIC-CORE HF score showed superior predictive ability and clinical benefit. Further research is needed to validate these models in diverse Asian populations.</p>","PeriodicalId":10492,"journal":{"name":"Clinical Medicine","volume":" ","pages":"100322"},"PeriodicalIF":3.9000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12145831/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/j.clinme.2025.100322","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/30 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The Atherosclerotic Risk in Communities (ARIC) heart failure (HF) score was originally developed in the USA to predict new-onset HF. Our goal was to validate the ARIC-HF score and develop a new score to predict HF in an Asian population.
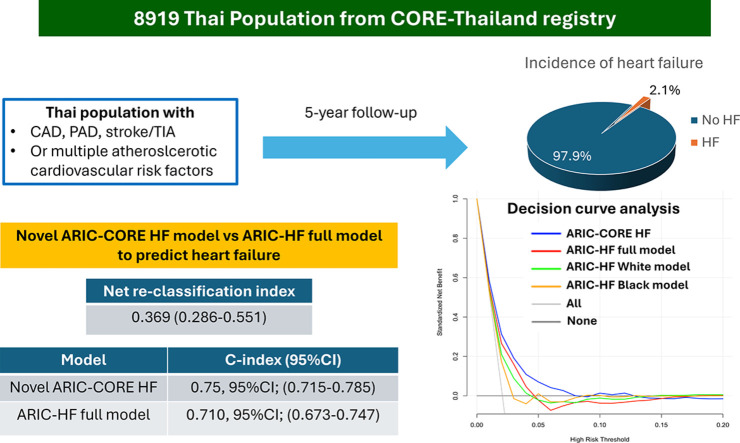
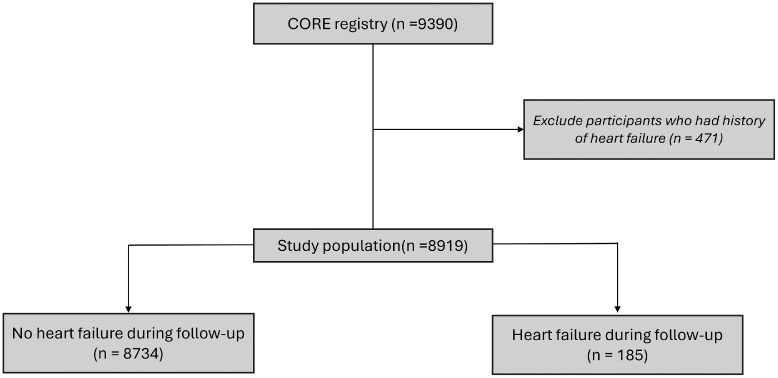
Methods: The Cohort Of patients with high Risk for cardiovascular Events (CORE-Thailand) was a prospective registry of Thai patients with high atherosclerotic risk. Patients were followed for 5 years for HF events. The ARIC-HF score was applied to predict HF. The new ARIC-CORE score was developed by re-estimating the coefficients of ARIC score variables using ridge regression. The discrimination and calibration of the models were assessed. The net reclassification index (NRI) was used to compare the prediction performance between the models. Clinical utility was assessed with a decision curve analysis.
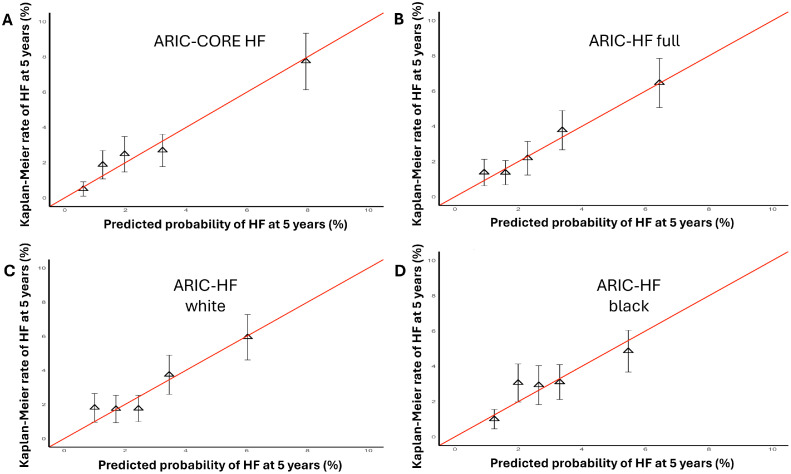
Results: From a total of 8,919 patients, 185 (2.1 %) developed HF. The ARIC-HF score and ARIC-CORE HF risk score provided good discrimination with C-statistics of 0.710, (95 % confidence interval (CI); 0.673-0.747) and 0.75, (95 % CI; 0.715-0.785), respectively. Both models showed a good calibration. Using the ARIC-CORE HF score was associated with an improved reclassification of HF (NRI 0.369, 95 % CI; 0.286-0.551) compared to the ARIC-HF score. The net clinical benefit of the ARIC-CORE HF score was higher than the ARIC-HF score in the decision curve analysis.
Conclusion: The ARIC-HF score performed well in predicting heart failure in the CORE population. The ARIC-CORE HF score showed superior predictive ability and clinical benefit. Further research is needed to validate these models in diverse Asian populations.
期刊介绍:
Clinical Medicine is aimed at practising physicians in the UK and overseas and has relevance to all those managing or working within the healthcare sector.
Available in print and online, the journal seeks to encourage high standards of medical care by promoting good clinical practice through original research, review and comment. The journal also includes a dedicated continuing medical education (CME) section in each issue. This presents the latest advances in a chosen specialty, with self-assessment questions at the end of each topic enabling CPD accreditation to be acquired.
ISSN: 1470-2118 E-ISSN: 1473-4893 Frequency: 6 issues per year

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


